서 론
괴사성 근막염(necrotizing fasciitis)은 표재성 근막의 감염에 의해 빠르게 진행되며 광범위한 연부조직의 괴사를 특징으로 하는 중증 감염성 질환이다. 외상이나 수술 이후에도 발생 가능하며 연부 조직이 있는 신체 어디에서든 발생할 수 있으나, 사지에서 가장 흔하게 발생하는 것으로 알려져 있다[1]. 괴사성 근막염은 국소 감염으로 시작되어 단시간 내에 근막 깊이까지 침투할 수 있으며, 평균 사망률은 25%에서 35%에 이르고, 치료가 지연되어 적극적 변연절제술(debridement)이 시행되지 않을 때에는 사망률이 70%에서 100%까지 증가할 수 있다[2,3]. 괴사 조직의 변연절제 후 남은 결손 부위의 창상 바닥(wound bed) 혈류 상태가 양호한 경우, 피부 이식으로 덮는 것을 고려할 수 있다[4]. 하지만 뼈의 노출이 있거나, 창상 바닥의 혈류가 좋지 않으면 치유의 지연으로 인해 기능적으로나 미용상으로 좋지 못한 결과를 낳을 수 있다.
본 증례 보고에서는 하지에 발생한 괴사성 근막염 환자에서 전경골근-근막피판(tibialis anterior musculofascial flap)과 부분층 피부 이식(split-thickness skin graft)을 이용하여 효과적으로 결손 부위의 재건을 시행한 사례를 소개하고자 한다. 본 연구는 헬싱키 선언의 원칙을 준수하였으며, 환자에게 사진촬영 및 사용에 대한 동의서를 취득하여 수행되었다.
증 례
특이 과거력 없는 61세 남성 환자가 우측 하지를 철제 구조물에 찔린 지 약 5일 뒤부터 발적과 통증을 동반한 염증 소견을 보였다. 이에 환자는 인근 정형외과 의원에 내원하였으며, 연조직염 진단 하에 세파제돈(cefazedone) 항생제 치료를 4일간 받았다. 그러나 창상은 호전되지 않았고 변색이 되었으며 수포가 형성되었다. 또한 염증 범위가 갑작스럽게 증가하였고, 혈압이 떨어지는 쇼크 증세가 발생하여 본원 응급실로 내원하였다. 환자는 패혈성 쇼크에 준하여 중환자실에 입원하게 되었고 경험적 항생제로 사이프로플록사신(ciprofloxacin)과 반코마이신(vancomycin) 치료를 받았다. 입원 후 촬영한 하지 자기공명영상에서, 전경골(anterior tibia) 부위의 궤양을 포함한 광범위한 피부 및 피하지방의 괴사 및 일부 비근(soleus muscle)과 비복근(gastrocnemius muscle) 사이의 근육간막(intermuscular fascia) 괴사 소견이 있었다. 창상에서는 메티실린 내성 황색포도알균(methicillin-resistant Staphylococcus aureus)이자랐고, 혈액검사상 C-반응단백 29.40 mg/dL, 백혈구 수 11,200 cells/mm3, 헤모글로빈 11.1g/dL, 나트륨 134 mmol/L, 크레아티닌 0.87 mg/dL, 혈당 70 mg/dL로 측정되어 LRINEC score(laboratory risk indicator for necrotizing fasciitis)가 7점으로 괴사성 근막염의 중간위험군(intermediate risk)에 해당하였다.
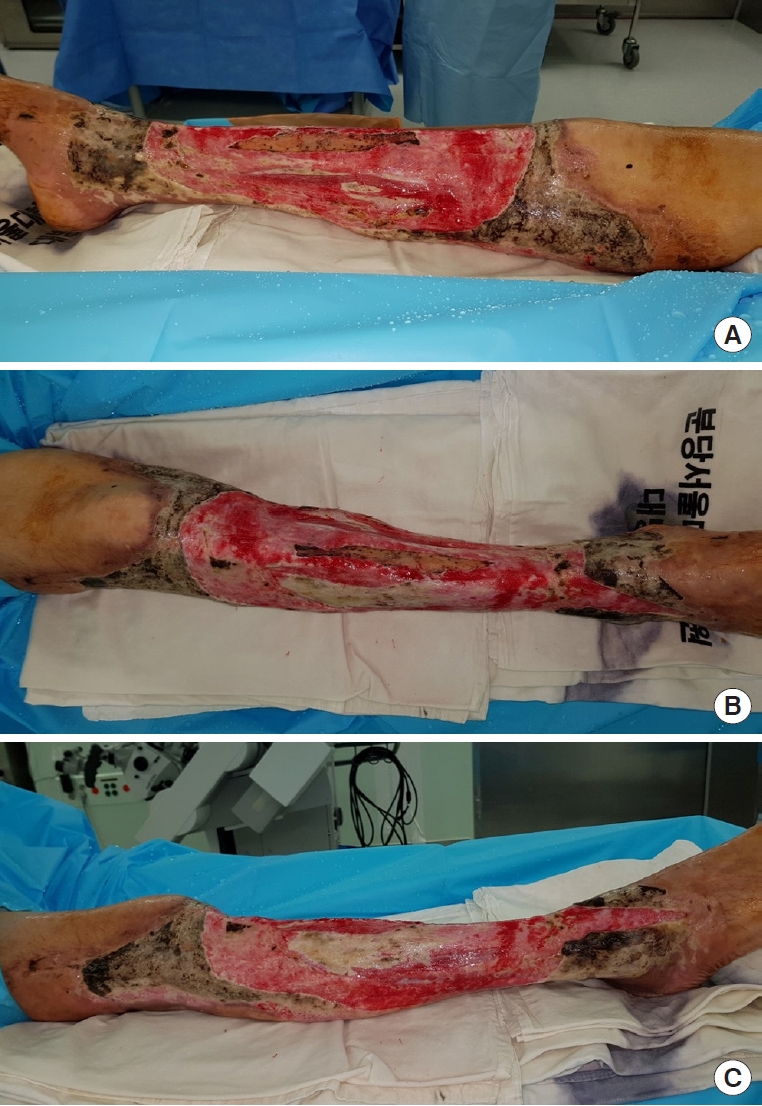
이에 괴사성 근막염 진단 하에 정형외과에서 응급 수술로 변연절제술을 시행하였으며, 이후에도 약 2주에 걸쳐 총 4회 변연절제술을 시행하며, 환자의 전신 컨디션은 서서히 호전되었다. 항생제로 사이프로플록사신과 반코마이신을 투약하던 중, 호중구감소증이 발생하여 반코마이신을 테이코플라닌(teicoplanin)으로 변경하였다. 환자가 응급실에 내원한지 약 1달 경과 후, 병변에서는 더 이상 균이 동정되지 않았으며, 혈액검사결과도 C-반응단백 3.5 mg/dL과백혈구수 8,600 cells/mm3으로 호전되었고, 창상에서 염증성 삼출물이 나오지 않았다. 감염내과 상의 하에 기존 항생제 투여를 중단하였고 박트림(Bactrim)만 투여하였으며, 우측 하지의 광범위한 연부조직 결손에 대해 재건 수술을 시행하기로 하였다. 하지의 창상은 무릎 부위에서 발목 부위까지 앞쪽 다리 전반부에 걸쳐 있었고 결손 부위의 크기는 약 30 × 20 cm에달하였다(Fig. 1).
재건에 앞서 변연절제술이 시행되었다. 환자를 앙와위 자세로 눕힌채, 피부 및 일부 괴사된 근막을 포함한 잔존 괴사 조직을 모두 제거하였다(Fig. 2). 변연절제술 시행 후, 초기 병변에서 궤양이 있던 전경골의 중간 약 1/3 부위가 20×4 cm 정도 노출이 되었는데, 이 부위를 덮어주기 위해 괴사성 근막염으로부터 비교적 안전하였던 전경골근근막 피판을 활용하기로 하였다. 먼저 전경골근 내측(medial)에 위치하는 전경동맥의 천공지(anterior tibial artery perforator) 3개를 도플러를 활용하여 찾은 뒤, 이를 혈관경으로 하는 “ㄷ”자 모양의 전경골근-근막피판을 디자인하였으며, 이어서 전경골근의 외측(lateral)에서부터 근육을 이등분(bihalving)하여 피판을 거상하였다. 피판 거상 시 근육에서 신선한 피가 나오는 것을 확인하였다. 이후 거상한 피판의 내측을 축으로 하여 피판을 회전문처럼 회전시켜 뼈가 노출된 부위를 덮어주었고(Fig. 3), 이를 긴발가락굽힘근(flexor digitorum longus muscle)에 고정해주었다(Fig. 4). 피부의 결손에 대해서는 반대 측 허벅지에서 채취한 부분층 피부를 활용하여 덮어주었고 이후 압박 드레싱을 가하였다(Fig. 5).
피판과 이식된 피부는 합병증 없이 모두 잘 생착되었다. 수술 후 15개월 뒤 마지막 외래 방문 시 환자는 발목 관절 운동 범위 제한 및 보행 장애가 없었으며, 특별한 불편감 없이 혼자서 일상생활이 가능하였다(Fig. 6).
고 찰
괴사성 근막염은 여러 차례의 변연절제술을 해야 하며, 문헌 고찰에 따르면 약 22%가 사지 절단을 수반하기도 한다[5]. 적절한 변연절제술과 안정적인 재건은 기능의 보존과 이차 감염의 방지를 위해 필수적이다. 임상적으로 발열, 부종의 빠른 진행 및 비함요부종(non-pitting edema), 짙은 적색의 경화(induration) 및 수포 등이 중요한 징후이며, 이어서 피부의 괴사로 이어진다[1,3,6]. 본 증례의 환자도 병변 부위의 범위가 갑자기 넓어졌고 피부가 변색되었으며 수포가 발생하였다고 호소하였다. 일반적으로 피부의 괴사가 발생하기 전까지 환자는 임상적으로 보이는 상태에 비하여 심한 통증을 호소하므로 진단에 어려움을 겪기도 한다[6]. 괴사성 근막염은 비스테로이드성 소염제(non-steroidal anti-inflammatory drug, NSAID) 혹은 스테로이드의 사용력, 최근 수술력, 간경화, 악성 종양, 면역 저하, 비만, 당뇨 등과 연관되어 있으며, 특히 당뇨병을 가장 흔히 동반한다[7,8]. 정확한 기전이 알려져 있지는 않으나, 이러한 요인들이 호중구의 기능을 저하시키고 사이토카인(cytokine) 분비를 변화시켜서 세균 감염을 빠르게 진행하도록 만든다고 알려져 있다[9]. 통증의 경감과 해열을 목적으로 사용한 NSAID가 염증 징후를 가리는 효과를 나타내어 진단을 늦추는 것 또한 병변의 진행을 야기하는 인자로 작용한다[10]. 또한, 흔하지는 않지만 본 증례에서와 같이 기저 질환 없는 건강한 성인들에서도 일상생활 중 입은 외상이나 화상이 괴사성 근막염으로 발전할 수 있다[1]. 많은 경우 피부 이식만으로도 괴사성 근막염으로 인한 결손의 재건이 가능하지만, 그렇지 않은 경우 유리피판을 이용하여 효과적으로 재건이 가능하며, 이에 대한 사례 보고는 과거에 많이 있었다[11-13]. 그러나 괴사성 근막염 환자들은 당뇨, 비만, 흡연력 등 유리피판의 성공률을 저하시킬 수 있는 동반 질환이나 위험 인자를 가진 경우가 많고, 특히 생체 징후가 안정되지 않은 환자에게 장시간의 수술은 그 자체만으로도 부담이 될 수 있다. 또한, 광범위한 염증 반응은 이차적으로 혈관에 손상을 가할 수 있음으로, 유리 피판술을 시행하면서 함께 고려해야 한다고 할 수 있다[13]. 이러한 환자들에서는 비복근 피판(gastrocnemius flap) 혹은 가자미근 피판(soleus flap)을 활용한 국소 피판술도 시행 가능하며, 특히 본 사례와 같이 전경골 중간 1/3 지점에 결손 부위가 위치한 경우 효과적인 재건 방법이 될 수 있다[11,14]. 하지만 이 역시 공여부에 추가적인 흉터가 남게 되며, 보행 장애를 일으킬 가능성이 있다.
저자들은 이미 개방되어 있는 결손 부위 내에서 재건을 효과적으로 시행할 방법을 모색하였고, 괴사 범위로부터 비교적 안전하였던 전경골근을 이등분하고, 거상한 피판을 회전문처럼 피벗(pivot) 시키는 방법을 사용하였다. 본 증례에서 활용한 전경골근-근막피판이 동반 질환이나 위험 인자를 가진 환자의 정강 부위의 재건에 있어 공여부 합병증 및 기능 저하를 최소화하면서, 비교적 간단한 술식으로 사용될 수 있으리라 생각한다.