Introduction
Dystrophic calcification (DC) is an atypical buildup of calcium salts in non-skeletal tissue often triggered by local tissue damage. While DC after burn injuries is not common, when it does occur, it primarily affects joint areas, with the elbow being particularly susceptible [1]. Although there are few published cases of extra-articular soft-tissue calcification associated with burn scars, such conditions can manifest after a long latency period, generally arising from non-healing ulcers related to the scars [2].
Diagnosis of post-burn calcification often occurs after a substantial delay, thereby heightening the risk of malignant transformation. DC possesses a high propensity for recurrence, especially if any residual calcification remains after resection. Consequently, complete wide excision of all calcium deposits and the overlying tissue followed by skin grafting is advised [2]. However, in cases where wide excision followed by skin grafting cannot be performed due to aesthetic reasons, patient preferences, or economic constraints, the exploration of alternative treatment options become pertinent. Given the limited effectiveness of non-surgical treatments, the quest for less invasive surgical alternatives is justified.
In this report, we describe an uncommon case of a patient with soft-tissue calcification in an extra-articular burn scar that developed after an extended latency period of 40 years. The lesion was successfully treated with skin-sparing marginal excision, with no recurrence after 3 years. This report aims to demonstrate that skin-sparing marginal excision can be a potent alternative to the traditional method of wide excision followed by skin grafting, effectively mitigating DC without subsequent recurrence. The study was approved by the Institutional Review Board of Seoul National University Bundang Hospital (No. #B-2306-833-701). A written informed consent has been obtained for this publication from the patient.
Case
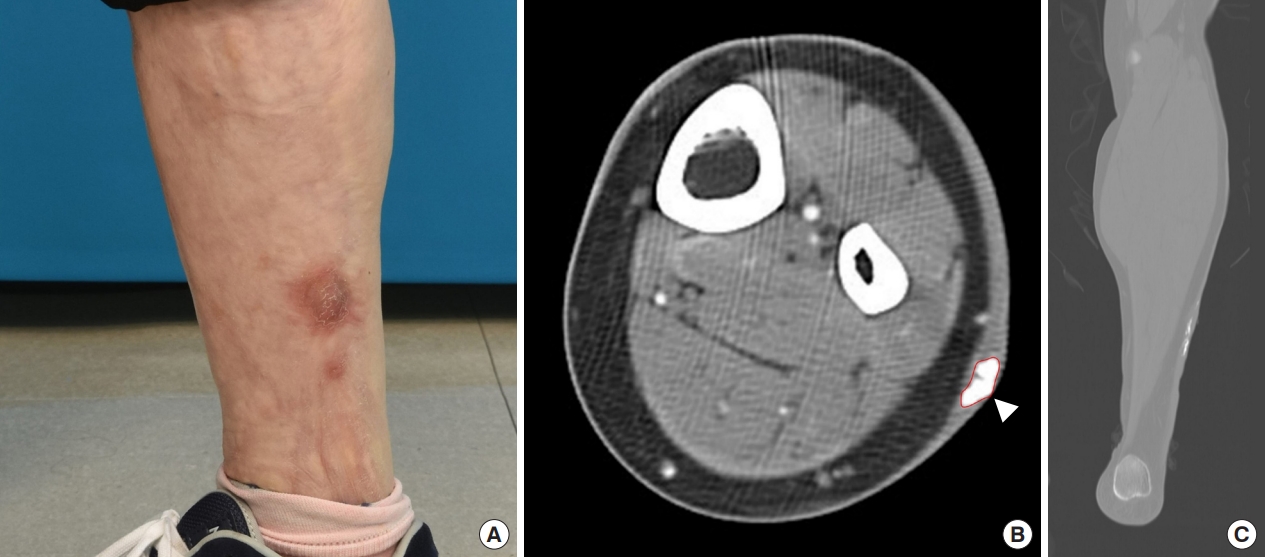
A 45-year-old female patient visited our clinic presenting a hypertrophic scar and an abscess-like lesion centered on her left lower leg, an area previously scarred from a burn injury suffered 40 years prior. Upon examination, a firm, 6 cm mass was observed at the base of a hyperpigmented scar on the anterolateral surface of the leg. The patient relayed a history of an ulcer producing a calcification-like discharge, which would heal secondarily, only to recur over subsequent years (Fig. 1A). Computed tomography scans showed dermal thickening and a 6.3×1.8 cm calcification within the intradermal layer (Fig. 1B and C). In addition, satellite calcifications were detectable near the main nodule. Blood tests revealed normal ranges for calcium and phosphorous levels, and there were no preexisting diagnoses of systemic connective tissue disorders. Based on radiographic and clinical findings, DC was suspected, leading to a recommendation of wide excision and skin grafting.
However, the patient declined this treatment, citing aesthetic and socioeconomic reasons. Thus, skin-sparing marginal excision was proposed and agreed upon, with the patient giving informed consent for regular follow-ups and accepting the potential for recurrence.
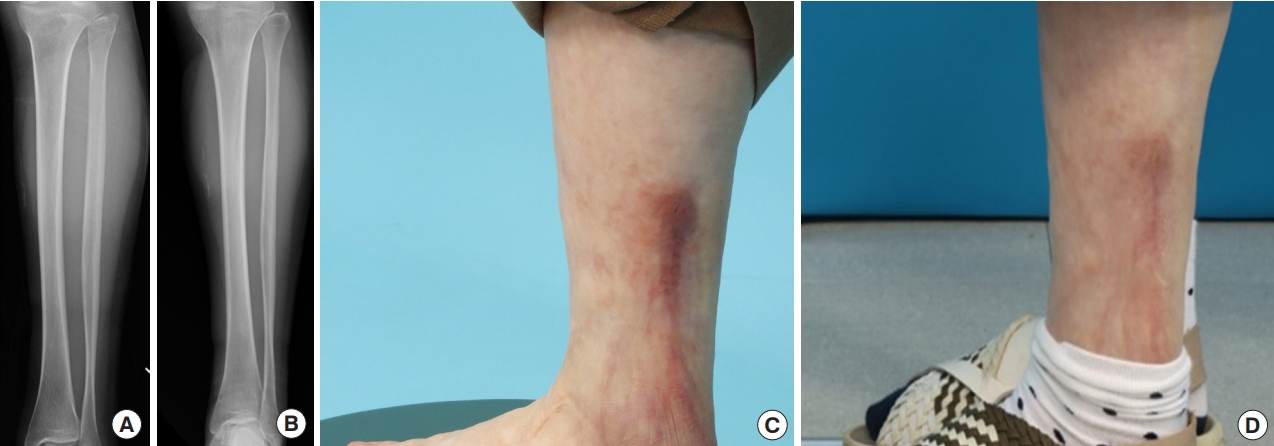
Ultrasound was used to guide preoperative marking of all calcified lesions. Subsequently, the primary calcified nodule (measuring approximately 6×1.8 cm) and satellite calcifications were meticulously excised (Fig. 2A). After excision, the overlying skin presented healthy blood perfusion and dermal bleeding, indicating that it was viable and could be preserved to allow for a tension-free closure. Histopathological examination revealed fibrous tissue with DC and surrounding hyalinization, characteristic of DC (Fig. 2B). Over a follow-up period of 3 years, which involved routine X-ray examinations every 3 to 6 months, no signs of recurrence were noted (Fig. 3A and B). The patient expressed satisfaction with her rapid recovery and the cosmetic appearance of the postoperative scar (Fig. 3C and D).
Discussion
DC is associated with various conditions, including trauma, burns, connective tissue disorders, infections, and radiation exposure [3]. DC is characterized by calcium deposits in tissues, despite normal serum calcium and phosphorus levels. It can also manifest in systemic disorders such as systemic sclerosis, dermatomyositis, and systemic lupus erythematosus [3]. The patient in our case did not display elevated serum calcium levels nor was diagnosed with any systemic disorder. These factors suggested that the DC originated from the burn sustained 40 years prior and the resulting scar tissue.
DC predominantly presents around joints and is an uncommon but recognized complication in burn patients [2]. Periarticular ossification can result in joint movement restriction and nerve compression, emphasizing the importance of early detection. In contrast, secondary soft-tissue ossification around ulcers takes longer to develop [4]. Since it is very rare for secondary soft-tissue ossification to occur after a burn, it is difficult to diagnose until overt symptoms such as ulceration are present. Even in rare cases, distinguishing these from chronic ulcers is challenging, given the usual absence of clinical symptoms such as restricted mobility, pain, swelling, or nerve paralysis. As a result, the diagnosis of ossification around ulcers takes a long time, increasing the possibility of malignant transformation.
The etiology of soft-tissue calcification following burn injuries remains poorly understood. Nonetheless, some hypotheses have been put forth based on limited research. Ramirez et al. [5] postulated that soft-tissue injury instigates the release of substance P by sensory neurons, which triggers mast cell degranulation and the ensuing inflammatory response. This inflammation recruits myeloid cells and lymphocytes to the injured tissue, leading to cell death. Inflammatory cells release cytokines, including BMP, thought to contribute to the calcification process [5]. Moreover, repeated local trauma across tight scars might cause punctate bleeding in the tissue, prompting focal changes conducive to calcium deposition [2]. Prolonged trauma, punctate hemorrhage, and hematoma formation secondary to the tearing of fibrous scar tissues might even trigger malignant transformation. It is crucial to distinguish these cases from Marjolin’s ulcer, a highly invasive squamous cell carcinoma [6]. DC can typically be differentiated from Marjolin’s ulcer by its smaller size, absence of soft tissue, lack of protruding edges, and the absence of cellular irregularity or malignant cells upon tissue examination [1].
In our case, several reasons led us to suspect DC rather than Marjolin’s ulcer. Firstly, the patient’s ulcer had not persisted continuously or enlarged since its onset and demonstrated a recurring pattern of ulceration and healing, leading us to consider DC rather than Marjolin’s ulcer. Secondly, during a previous ulcer episode, the lesion remained relatively small (<2 cm) and showed no significant margin protrusion or cellular irregularity. Furthermore, the ulcer was relatively shallow, lacking the deep penetration characteristic to Marjolin’s ulcer, and healed secondarily without further intervention. Considering these factors, a preliminary diagnosis of DC was made during the outpatient visit, distinguishing it from Marjolin’s ulcer. The pathological examination confirmed the absence of malignant cells and diagnosed DC.
There is ongoing debate on the optimal treatment of DC, with no standard algorithm available. Non-surgical interventions, including carbon dioxide laser or intralesional triamcinolone administration, may be considered. However, evidence regarding their efficacy is sparse. Laser treatment alone may not achieve sufficient removal, leading to a higher risk of recurrence. Intralesional injections may be limited by inadequate penetration into scar tissue [7]. Surgical excision has traditionally not been favored due to the heightened risk of delayed wound healing, infection, and potential impairment to the range of motion [8]. Nevertheless, in patients with limited response to non-surgical treatments, surgical excision should be considered for the management of DC.
DC is prone to recurrence if any amount of calcification remains post-surgery [2]. Additionally, chronic pressure in the affected area can facilitate calcium deposition. To reduce chronic pressure and minimize the risk of recurrence, a complete wide excision of all calcium deposits and the overlying skin followed by skin grafting is recommended [2]. However, alternative treatments should be considered when a patient refuses wide excision for personal reasons.
In our case, with preoperative and intraoperative ultrasound localization of all calcified lesions, it was possible to completely and thoroughly remove all of them. Moreover, by preserving the overlying skin, a tension-free wound closure was achieved, alleviating the pressure believed to be a precipitating factor of DC. Owing to peri-calcification dermal thickening, the overlying skin preserved after calcification resection had a low risk of necrosis. In cases where diminished skin perfusion is suspected, additional imaging such as thermography and indocyanine green fluoroscopy can be utilized to accurately assess skin perfusion and minimize complications. Furthermore, skin-sparing marginal excision can yield better aesthetic outcomes compared to performing wide excision followed by skin grafting. Frequent follow-up visits and X-ray examinations were scheduled to detect any recurrence early.
Over a 3-year observation period, we noted no recurrence of calcifications or ulcers, including in radiographic examinations. This case suggests that if a patient maintains good compliance and can attend regular outpatient clinic visits for imaging and physical examinations, skin-sparing marginal excision could be a viable alternative to wide excision and skin grafting for patients with DC. We propose that even in cases where the lesion size is large, or the calcification is diffuse and deep, it is possible to consider management through skin-sparing marginal excision followed by primary closure. Delicate removal of the calcification lesion using guiding techniques such as ultrasonography, without leaving any remnants, and excising only skin involved in open wounds while preserving the rest of the overlying skin can reduce skin tension and alleviate the chronic pressure which is a triggering factor for DC. We believe this approach can be attempted for cases with larger or more diffuse lesions, or cases where the calcification depth is significant.
Furthermore, the lower extremity is well-known to be more prone to calcification due to the higher frequency of microtrauma [7]. Therefore, providing patient education on avoiding additional triggering factors (such as pressure, trauma, etc.) around the affected site after surgery can aid in reducing the recurrence. However, given that this is a single case report, it is crucial to apply this approach to a broader range of cases and observe the outcomes before establishing this method as a standard treatment protocol for DC.