Introduction
Angiosarcoma is a rare soft tissue sarcoma accounting for less than 2% of all soft tissue sarcomas [1]. It is an aggressive malignant neoplasm originating from the endothelial cells of blood or lymphatic vessels. While it occurs most commonly in the head and neck region, it can be located in any anatomical site of the body [1,2]. The cutaneous form of angiosarcoma is characterized by diffuse and ill-defined margins, which complicate surgical management [3,4]. It is also associated with a high rate of local recurrence and distant metastasis to other organs [5]. The extensive skin and subcutaneous tissue involvement is due to its tendency toward horizontal spread, with progression of the tumor along vascular structures [1,6]. For these reasons, cutaneous angiosarcoma has poor prognosis with a 5-year survival rate ranging from 30% to 40% [7]. Aiming at a clinical demonstration of this rare tumor, we report a case of cutaneous angiosarcoma located in the scalp, presenting as facial cellulitis which was aggravated by hair dyeing. The report was approved by the Institutional Review Board of Soonchunhyang University Hospital (IRB No. 2021-02-051) and informed consent for publication of the study was obtained from the patient.
Case
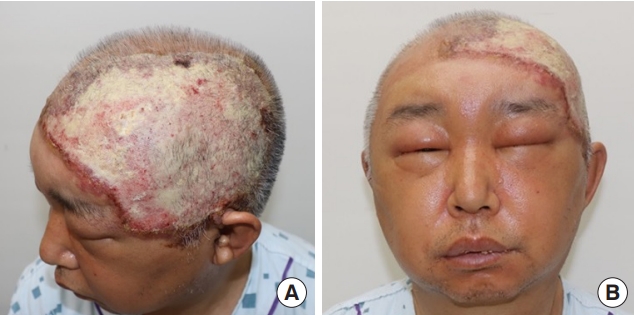
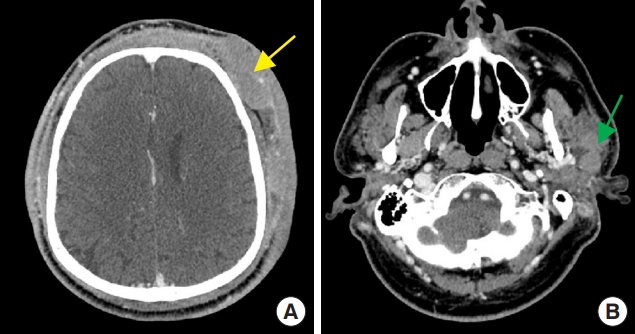
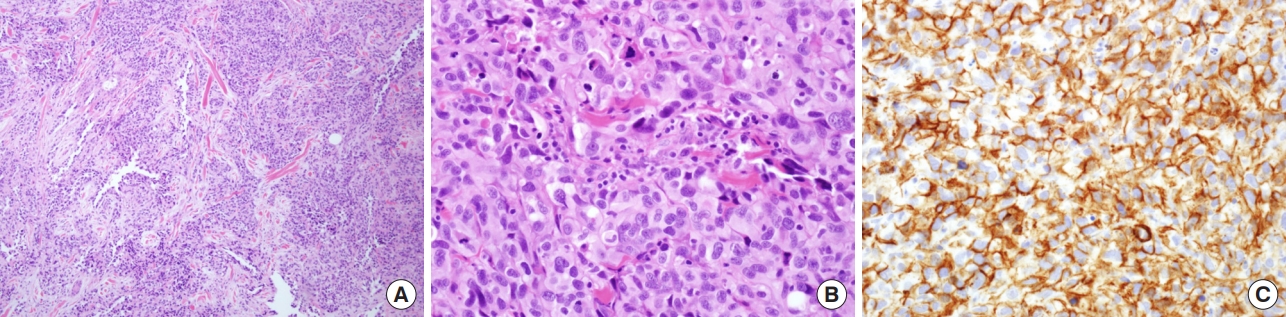
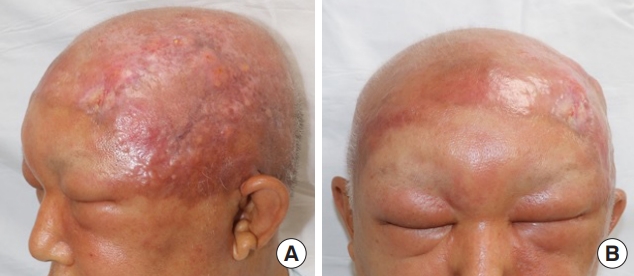
We report a case of a 55-year-old male patient who had no significant past medical history. Since he had dyed his hair 3 months before his visit, an ulcerated lesion with turbid discharge occurred on his scalp. He came to the emergency room because of bilateral swelling and redness of the whole face with a 15×10 cm-sized ulcerative scalp wound that had gradually grown in size (Fig. 1). The patient had been treated with oral antibiotics for 2 weeks after a single dose of empirical intravenous cefazoline in a local clinic. Nevertheless, the lesion worsened and the patient was admitted to the department of infectious medicine and given terbinafine 250 mg per day for a week for a possible tinea capitis or another fungal infection. However, there was no improvement in his facial swelling and redness. On facial enhanced computed tomography (CT), several potentially malignant lymph nodes and parotid gland enlargement were found together with the bilateral facial cellulitis (Fig. 2). Under general anesthesia, incisional biopsy was performed from multiple sites on the scalp skin, parotid gland tissue and parotid lymph nodes (Lt level VIII) (Fig. 3). Debridement of inflammatory and unhealthy tissue was also carried out with bacterial culture of the inflamed tissue around the suspected cancer lesions on the scalp and preauricular area.
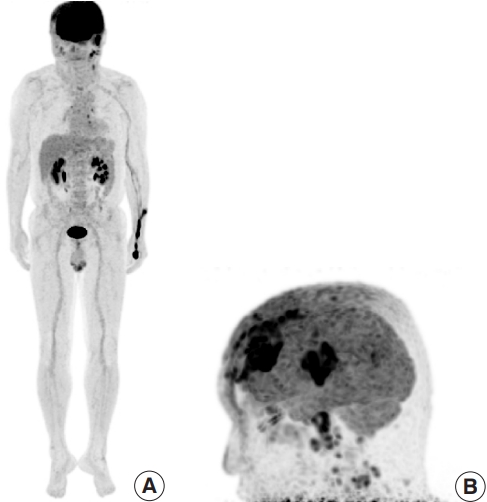
After surgical debridement with multiple incisional biopsies, a diagnosis of scalp angiosarcoma with metastasis to parotid gland and lymph nodes was confirmed (Fig. 4). Stenotrophomonas maltophilia and Helcococcus kunzii, opportunistic infections that can occur in immunosuppressed patients, were identified from bacterial cultures of inflamed tissue [8,9]. For staging workup, magnetic resonance imaging (MRI) of the neck was performed, revealing multiple enlarged lymph nodes suspicious of malignancy in the parotid gland and both level II and V of the neck. No distant metastasis other than in the head and neck region were identified on positron emission tomography-CT, chest CT, abdominopelvic CT, and bone scan (Fig. 5). Considering the stage and unresectable status of the cancer, chemotherapy was planned, and the wound of the scalp lesion was managed conservatively by daily dressings with antibiotic topical agent and foam. Although the facial swelling improved only slightly, the wound infection stabilized, and the patient was discharged.
Following up for outpatient treatment, chemotherapy with paclitaxel was performed for 12 weeks as a first line therapy. Additionally, palliative radiotherapy consisting of 4.0 to 5.0 Gy per fraction with a total dose of 65 Gy to the scalp lesion and left cheek was performed (Fig. 6). Although facial swelling persisted, the scalp wound was stabilized without any discharge (Fig. 7). Afterwards, second-line chemotherapy using adriamycin was performed three times with palliative radiotherapy involving 4.0 Gy per fraction with a total dose of 60 Gy. Ulcerative lesions due to irradiation reoccurred on the scalp but were successfully managed with self-dressings using foam.
Discussion
Angiosarcoma is a highly aggressive malignant tumor originating from vascular endothelial cells, which takes up below 2% of all soft tissue sarcomas [1]. It ranges from well-differentiated tumors which have inherent properties of normal epithelium to poorly differentiated tumors [6]. While angiosarcoma can originate from any anatomical location including skin, soft tissue, bone, breast, and other visceral organs, it manifests dominantly as cutaneous lesions [10]. Although most soft tissue sarcomas are located in the deep layer of soft tissue under the skin, angiosarcoma mainly presents at the dermis and may extend to the superficial soft tissue [6,7].
The cutaneous form of angiosarcoma most commonly occurs in the head and neck region, especially the scalp. The clinical appearance of cutaneous angiosarcomas varies greatly according to individual cases. It is necessary to differentiate cutaneous angiosarcoma from other types of skin cancer such as melanoma or squamous cell carcinoma considering its non-specific morphologic properties [11,12]. Cutaneous angiosarcoma can manifest as a single lesion or multiple lesions; with a bluish or violaceous color; including nodules, plaques, or flat infiltrating areas; and is occasionally accompanied by bleeding or ulceration [4,5]. In the early stages, it usually occurs with the clinical appearance of a bruise-like lesion with an indistinct border, but in advanced lesions, it can progress to being nodular, elevated, or ulcerated [6]. On the scalp, early lesions can be hidden in the hair, making early detection difficult [13]. Thus, as the primary lesion aggressively progresses, it could be mistaken for tinea capitis or facial cellulitis due to infection accompanying the cancerous lesion or lymphedema in surrounding tissues [3,6]. Being an immigrant from China, this particular patient made a delayed visit to the hospital because his status rendered health care less accessible. The infection of the scalp lesion was quite advanced, leading to facial cellulitis, and this confused the diagnosis. Furthermore, the patient had applied hair dye without being aware that a malignant cutaneous lesion was in his scalp. More than three-fourths of hair dye products are oxidizing agents which irritate the skin and can even cause infections such as contact dermatitis in severe cases. It is possible that the patient had cutaneous angiosarcoma lesions with raw surfaces, which were made worse by irritation from the hair dye. Because enhanced facial CT revealed abnormal findings in the lymph nodes, we performed excisional biopsies in multiple sites involving the primary scalp lesion.
In this case, angiosarcoma was confirmed on biopsies of the skin of scalp and parotid gland, which was FNCLCC (Fédération Nationale des Centres de Lutte Contre Le Cancer) grade 3. Immunohistochemical staining results were positive for CD34 and CD31 with 70% to 80% of Ki-67. Enhanced neck MRI indicated multiple metastatic lymph nodes in the parotid gland and both sides of the neck. It was difficult to resect all of the cancerous lesions as they were widely dispersed on the scalp with regional metastasis to the cervical lymph nodes and parotid gland. Chemotherapy with paclitaxel was performed as first-line therapy over a duration of 12 weeks. Severe swelling due to lymphedema of the whole face necessitated palliative radiation therapy. Follow-up radiological examination was performed every 3 months, and second-line chemotherapy with adriamycin was administered with the palliative radiation therapy. During this period, the patient was receiving regular dressings for the primary ulcerative scalp lesion. In the process, the lesion worsened due to irradiation, but gradually improved with foam dressings.
In conclusion, the varied appearance of cutaneous cancerous lesions of the scalp complicates early detection, as does its anatomical location which is covered with hair follicles [1]. Additionally, cutaneous cancerous lesions on the scalp can be mistaken as facial cellulitis, because they can progress aggressively with lymphedema in surrounding tissues and infection of the cancerous lesions. This applies to malignant skin tumors like squamous carcinoma cell or basal cell carcinoma as well as cutaneous angiosarcoma, suggesting that scalp lesions need to be carefully observed. Finally, it should be noted that soft tissue sarcomas are aggressive; this case demonstrates the importance of excisional or incisional biopsy for early detection of primary cutaneous angiosarcoma and the possibility of its misdiagnosis as facial cellulitis after infectious events such as using hair dye.