Introduction
The development of pressure injuries (PIs) is used as an indicator of nursing care quality [1] because it is the most serious manifestation of impaired skin integrity. PIs are associated with morbidity or mortality from various diseases in hospitalized patients and cause an increase in the duration of hospital stays [2]. Even though hospitals assess risk groups for PIs, prevent them according to standardized PI guidelines and apply advanced products and technologies for wound care, the incidence of PIs has not decreased. This is because factors such as population aging and increased chronic underlying diseases make PIs inevitable [3]. Many studies on the degrees of PI healing have been conducted due to the increased importance of PI treatment.
For the treatment of PIs, it is most important to relieve pressure from the PI area, remove necrotic tissue to promote development of granulation tissue, and provide adequate hydration. Dressings of various materials are used for PI management to achieve these goals, among which polyurethane foam is particularly useful because it can absorb excess exudate and keep the PI area moist while reducing external pressure [4]. Meanwhile, PIs are by definition ischemic areas that do not receive nutrition, oxygen, immune cells, antibodies or antibiotics normally, and are made more susceptible to infection by neurological disorders [5]. Chronic wounds including PIs do not easily show symptoms of acute infection; the symptoms are noted only when the infection is chronically advanced [6]. On the other hand, chronic wounds such as PIs are very frequently colonized to a certain extent. As a result, biofilms can easily form on PIs and deteriorate into local infection or spread to become a systemic infection [7], so reducing the bacterial load is essential [8]. In particular, infection should be suspected if the area where a PI frequently occurs is close to the perianal region or buttocks, where contamination from feces can repeatedly take place [9], and where there is always the potential to progress to an infection [10]. Therefore, if microorganisms colonize the wound or delay wound healing, antiseptics or antibacterial dressings should be used [11].
However, since most antimicrobial dressings available in Korea are expensive imported silver dressings, less costly dressings containing antimicrobial agents such as povidone-iodine (PVP-I), an antiseptic that is commonly used in Korea, are needed. While 10% PVP-I is a commonly used antiseptic for infected wounds, it can inhibit the growth of new tissue when used on open wounds. However, if an equilibrium is established in the composition, concentration and temperature of a povidone-free iodine composition, problems associated with skin exposure to early iodine components can be minimized [12]. A meta-analysis of an in vivo study also found that PVP-I may delay wound healing in the early stages of use, but as the overall total time for healing is not affected, the Wound Healing Society and the Japanese Pressure Ulcer Advisory Panel tend to allow the use of PVP-I [13]. Recent studies on the efficacy and safety of a foam dressing containing 3% PVP-I foam reported that among several different types of dressings, 3% PVP-I foam dressings best promoted wound healing based on the rates of re-epithelization, new blood vessel formation, collagen deposition, and permeation of antimicrobial agent into tissues [14-16]. In light of these results, this study was designed to evaluate the efficacy of 3% PVP-I foam dressings for the treatment of PI lesions compared to silver foam dressings. In this non-inferiority trial, 3% PVP-I foam dressing (Betafoam N, Genewel) and silver foam dressing (Mepilex Ag, Mölnlycke Health Care) were applied to PI subjects to compare the efficacy of PI healing in terms of the degree of healing, reduction of wound size, and the time to heal.
Methods
Study design and subjects
This prospective randomized non-inferiority trial to evaluate the utility of a 3% PVP-I foam dressing for PI treatment was conducted between April 2016 and December 2019 at three sites in South Korea. Subjects with PIs on their buttocks were assessed for eligibility based on the following key inclusion criteria: age ≥19 years; no dermatitis or ischemic disease throughout the body or PI area; no clinical symptoms of local infection at the PI site; PI size ≥1 cm2; PI stages 2, 3, or 4 (only stage 4 PIs which had recently turned into stage 4 were included); no chronic hyperglycemia (blood glucose level <200 mg/dL or hemoglobin A1c ≤7); and stable vital signs allowing the patients to change position every 2 hours. The main exclusion criteria were hypersensitivity reactions to PVP-I or silver.
For selection, a screening number was assigned to each subject, and after completing all screening processes, if the subject was found suitable for this study, a random assignment number was sequentially assigned, and Betafoam N was applied to the experimental group while Mepilex Ag was applied to the control group. The screening numbers and randomization numbers for subjects who dropped out of the study were also removed together with the corresponding subjects and not re-assigned to new subjects. New subjects were assigned a new subject screening number and randomization number. This study was approved by each Institutional Review Board (2015-06-123, 2016-07-035, 2017-04-003), and all subjects participated in this study after providing written informed consent.
Study procedures
Demographic and pertinent clinical data were collected from the subject’s medical records or through direct assessment. This included sex, age, major diagnosis, classification of PI, Pressure Ulcer Scale for Healing (PUSH) score, and Image J score. The subjects were also evaluated by the Braden scale score, body mass index, hematological tests, vital signs, the use of vitamins or steroids, use of vasopressor for >48 hours, use of any support surfaces or devices, and ability of regular repositioning. The Malnutrition Universal Screening Tool developed by the Malnutrition Advisory Group of the British Association for Parenteral and Enteral Nutrition for nutritional as sessment was used to evaluate nutritional status. Past medical history was checked for PI history, diabetes and hypertension, and the presence of urinary and fecal incontinence. PIs were categorized into six classifications according to the National Pressure Injury Advisory Panel, and only stage 2 to 4 PIs were included in this study. The PUSH tool developed by National Pressure Injury Advisory Panel was used to evaluate the degree of PI healing and time to heal by observing three variables: ulcer size (1–10 points), exudate (1–3 points) and tissue type (0–4 points). Afterwards, the three subscale scores were added up to generate a cumulative wound status score. The total score is between 0 and 17 points, and a larger score indicates a more severe PI condition. PUSH tool measurers were trained for 1 hour using PowerPoint and printed materials before the study. Afterwards, they were shown five cases on a computer and evaluated the tool’s intraclass correlation of 0.96. The degree of PI size reduction was confirmed before and after the study using an Image J program developed by the National Institute of Health. The time to heal was analyzed using PUSH scores.
The subjects were evaluated through the PUSH tool, Image J score, and blood tests by one wound ostomy continence nurse (MK) in the initial stage. The dressings for both groups were changed by the unit’s nurses every 3 days, for up to 8 weeks (cases of complete healing were excluded from dressings), and subjects who withdrew before 8 weeks (deaths, disability to change position, terminal cases giving up on treatment, cessation of participation, surgery, and discharge) had their dressings changed until they dropped out. At the end of the study, the wound ostomy continence nurse evaluated the PUSH score and Image J score. All subjects received our facility’s standard PI preventive care bundle that included turning and repositioning every 2 hours, regular skin cleansing and application of a skin protectant, etc.
Statistical analyses
The sample size was determined using a method of calculating the number of non-inferiority binary variable samples. Statistical significance was set at 5%, and the power was set at 80% using a 1:1 group size ratio and 2-sided tests. Based on the literature [9], a PI healing rate of 80%, up to 12% difference in healing rates between the two groups [17], and a drop rate of 20% was predicted. It was determined that a total of 80 cases, 40 cases in each group, were to be included in the study.
Data were analyzed using the SPSS software program version 22.0 (IBM Corp.). The demographics, characteristics related to PI, and homogeneity of the two groups were compared using chi-square test or independent t-test, analysis of variance, Fisher exact test, and Fisher-Freeman-Halton exact test. The degree of PI healing was analyzed using a chi-square test, the degree of reduction in PI size was analyzed using an independent t-test, and the time to heal was analyzed using Kaplan-Meier survival analysis in the experimental group (3% PVP-I foam dressing) and control group (silver foam dressing). To prevent attrition bias and reflect the intention to treat, 80 subjects including all dropout subjects were analyzed and missing values were treated statistically.
RESULTS
Disposition and baseline characteristics of subjects
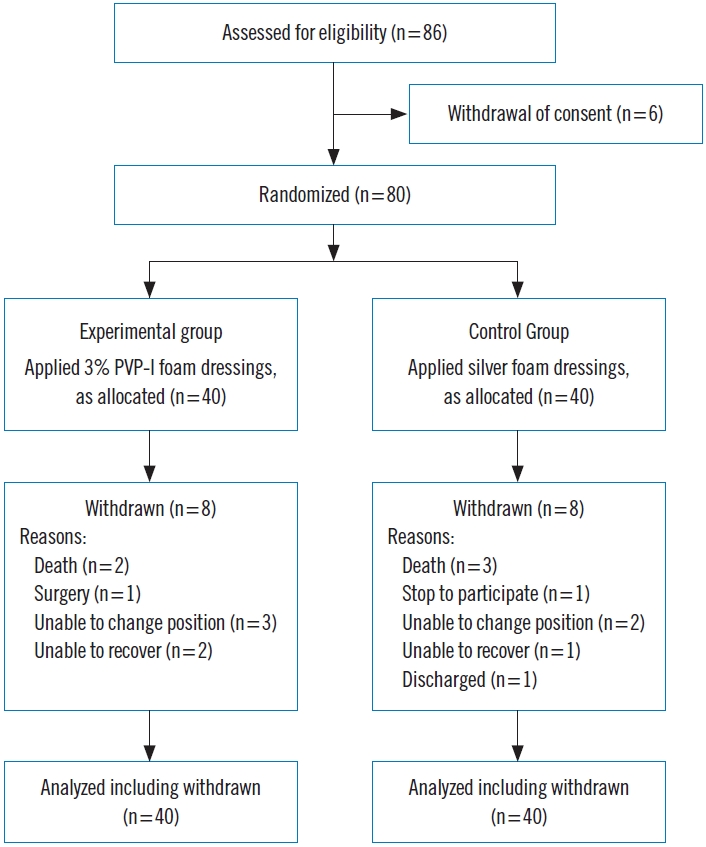
Initially 86 subjects were screened, and six subjects who withdrew their informed consent were excluded. A total of 80 subjects, 40 subjects in each group, were enrolled including 16 sub-jects (five deaths, five unable to change position, three giving up treatment due to unrecoverable terminal status, one renouncing participation, one surgery, and one discharge) who withdrew during the study. The subjects’ data was then analyzed (Fig. 1). The average age of subjects was 62.7±13.4 years in the experimental group and 65.7±15.3 years in the control group. In the classifications of PIs, there was no statistical difference between the two groups, with 22 (55.0%) and 18 (45.0%) in PI stages 2 and 3, respectively, in the experimental group; and 26 (65.0%) and 14 (35.0%) in the control group (χ2= 0.833, P=0.361), respectively. The homogeneity of the two groups was analyzed using a chi-square test or independent t-test to compare demographics and PI-related characteristics. No significant differences were found between the two groups (Table 1).
Intervention effect
The efficacy of PI healing was evaluated by three measures: the degree of healing using PUSH, the degree of reduction in PI size using Image J, and the time to heal using the Kaplan-Meier survival analysis.
First, for the degree of healing based on PUSH, subjects from the two groups with 70%, 50%, and 30% degrees of healing were compared based on PUSH scores. In the experimental and control groups, 25.0% (10 cases) and 17.5% (7 cases), respectively, healed by more than 70% (χ2=0.743, P=0.389); while 32.5% (13 cases) and 42.5% (17 cases), respectively, healed more than 50% (χ2=0.891, P=0.345); and 55.0% (22 cases) and 67.5% (27 cases) respectively healed more than 30% (χ2=1.338, P=0.247). There was no statistically significant difference between the groups (Table 2). Second, the degree of reduction in wound size was measured using Image J (1.52a) to analyze the difference in the PI size before and after treatment. The experimental and control groups decreased by 41.6%± 35.3% and 49.7%±38.2%, respectively, demonstrating was no statistically significant difference (χ2=–0.986, P=0.327). Third, the Kaplan-Meier survival analysis to confirm the time to heal showed that if more than 30% of the PUSH score was healed, the time to heal was 27.0±9.3 days for the experimental group and 18.0±2.8 days for the control group, but there was no significant difference between the two groups (χ2=3.225, P= 0.073). The healing rates at 50 days were 85.8%±8.9% and 93.9%±5.7% in the experimental and control groups, respectively (P=0.073), but there was no significant difference between the two groups (Fig. 2). No complications from the application of dressings were observed in either group.
Discussion
This study is the first non-inferiority study on PIs designed to compare the efficacy of two antimicrobial dressings (3% PVP-I foam dressing and silver foam dressing) based on the degree of healing, the degree of reduction in wound size, and the time to heal. Notably, none of the subjects had a PI infection during the study period. The degree of healing was not significantly different between the treatment groups, and neither were the degree of reduction in wound size and the time to heal in both groups significantly different.
A variety of wound dressings are available in clinical practice, designed to absorb and retain wound exudate while maintaining a moist wound environment for optimal healing [18]. Among the various dressing materials, polyurethane foam dressings are widely used due to their excellent management of exudates and ability to protect wounds from invasive microorganisms. Recently, foam dressings have been shown to be able to play a role in transporting antimicrobial agents, which has led to the use of many different types of foam dressings, including silver or other bactericidal agents. Silver foam dressings have been frequently used to heal wounds, including PIs, burns, and diabetic wounds, which are susceptible to contamination or infection [15]. Since clinical experience has demonstrated the antimicrobial effects of silver dressings, silver has been used in various forms and various types of dressings. However, several studies have demonstrated side effects related to silver. One study proved that silver has a cytotoxic effect on the wound bed and is deposited in organs, which inhibits the growth of human fibroblasts, delaying wound healing [19]. The use of silver dressing requires careful attention because reactive oxygen species induced by using silver are highly reactive and cause oxidative DNA damage and inflammation [20].
Meanwhile, PVP-I is an antiseptic agent commonly used as a water-soluble complex with iodine elements bound to synthetic polymers and can be applied to various types of wounds, including PIs, abrasions, lacerations, and skin infections. Recently, PVP-I products have been developed on the study-proven premise [15] that the antimicrobial activity of PVP-I contained in dressings is level to that of silver contained in dressing products, but with a reduction in cost and cytotoxicity. Although current studies related to the cytotoxicity of PVP-I are conflicting, some articles have reported improved wound healing using PVP-I [21]. The Wound Healing Society and the Japanese Pressure Ulcer Advisory Panel also recommended the use of different lower concentrations of PVP-I [13]. One current study by Lee and Song shows that 3% PVP-I foam dressing was the most effective dressing for wound healing and re-epithelialization compared to the many types of silver foam dressings and gauzes [15]. Although the mechanism is still unclear, the 3% PVP-I foam dressing group demonstrated significantly more neoangiogenesis and deposition of collagen depositions than other groups. Mechanical trauma should be minimal when changing dressings and cleansing wounds since trauma to the wound bed delays wound healing. Accordingly, when DNA remaining in the dressings at 3, 7, 10, and 14 days was examined to investigate the degree of tissue damage during dressing changes, the 3% PVP-I foam dressing group had less separation of tissue than any other group [15].
In our study, there was no significant difference between groups in degrees of healing, wound size reduction, or time to heal. In addition, it was proven that the healing efficacies of the 3% PVP-I foam dressing and silver foam dressing were similar.
In the 2018 in vivo study by Lee and Song [15] applying 3% PVP-I foam dressing and several other dressing agents (Allevyn Ag, Polymen Silver, Mepilex Ag, Medifoam Silver, and Gauze) to full-thickness rat wounds, the wound size was most noticeably reduced in the 3% PVP-I foam dressing group with a significant difference from the other groups by day 14. Pak et al. [16] reported the percentage of complete epithelialization and wound infection in split-thickness skin graft donor sites on postoperative day 14. The full epithelialization time was shortest with 3% PVP-I foam dressings (12.74±3.51 days) compared to hydrocellular foam dressings (16.61±4.45 days; P=0.0003) and petrolatum gauze (15.06±44.26 days, P=0.0205). On day 14, 83.87% of the 3% PVP-I foam dressing donor sites displayed complete epithelialization, while 36.36% (P=0.0001) of hydrocellular foam dressing donor sites and 55.88% of petrolatum gauze donors had completed epithelialization. Additionally, the PVP-I foam dressings tended to improve exudate management by causing less bleeding and adherence on the wound bed, resulting in less exudate leakage. The superior fluid-handling capacity of PVP-I foam dressings has also been demonstrated in another previous study [22].
Because cases have been reported in which other antibacterial agents containing silver cause allergic reactions to human skin when used for a long time, further research will be required on whether 3% PVP-I foam dressings cause allergic reactions or microbial resistance on the skin with long-term use [14]. In addition, future studies should be conducted to confirm whether 3% PVP-I foam dressings have the effect of healing PIs even when applied to subjects in long-term care settings or with various clinical wounds. While dressing change intervals depend on wound conditions, manufacturers generally recommend a dressing change interval of up to 3 days for 3% PVP-I foam dressings and up to 7 days for silver foam dressings. However, in terms of cost effectiveness, the price of a 3% PVP-I foam dressing is about a quarter of the price of a silver foam dressing, and while silver dressings are not currently allowed for PI treatment by the national health insurance system in Korea, 3% PVP-I foam dressings have the advantage of being covered by national insurance for PI treatment. Therefore, a more comprehensive analysis is needed to evaluate the potential cost savings associated with using 3% PVP-I foam dressing, including the cost of dressing changes.