Introduction
The number of patients receiving cardiac implantable electronic devices (CIEDs) is steadily increasing worldwide [1]. Patients who receive implantation or replacement of CIEDs such as pacemakers, implantable cardioverter-defibrillators (ICD), cardiac resynchronization therapy pacemakers (CRT-P), and CRT defibrillators (CRT-D) are often on anticoagulation and antiplatelet therapy, as they carry a high risk for severe comorbidities [2]. Pocket hematoma is the most common complication after CIED procedures, with an overall incidence of up to 15% in some patient subgroups [3-5]. Pocket hematoma is associated with factors such as patient age, comorbidities, use of anticoagulant and antiplatelet drugs, device type, implantation procedure type, and the surgeon’s experience. There is a 9-fold increase in the risk of infection in patients with pocket hematoma compared to those without pocket hematoma [6]. Moreover, CIED-related infection is among the most severe complications of CIED therapy, leading to substantially increased morbidity, prolonged hospitalization, elevated mortality risk, and additional healthcare costs [7,8]. There is no specific treatment for pocket hematoma once it occurs. Pocket hematoma is generally managed conservatively as long as it is not severe, requiring evacuation or CIED removal surgery.
Aspiration of hematoma is not a recommended treatment because it can lead to infection [6,9]. According to device registry data, early reoperation for hematoma or lead dislodgement is reportedly the strongest risk factor for CIED infection [10,11].
The present study aimed to explore whether lowering the infection risk by aseptically removing the hematoma at an early stage would be possible through aspiration. We also aimed to investigate the effectiveness of treatment with aspiration for pocket hematoma.
Methods
The charts of a total of 570 patients who had CIED implantations or replacements including pacemakers, ICD, CRT-P, and CRT-D implantation or replacement at our hospital between January 2011 and January 2021 were retrospectively analyzed. After the CIED procedure, a plastic surgeon performed wound closure in layers. When the patients were hospitalized right after undergoing the CIED procedure, a plastic surgeon and a cardiologist followed up on the patient together for pocket hematoma formation until they were discharged without any complications.
Following patient discharge, a cardiologist followed up on the patients at the outpatient clinic. If the outpatients developed a pocket hematoma, the cardiologist consulted with and referred the patients to the plastic surgeon. Thereafter, the plastic surgeon followed up with the patients until the hematoma resolved.
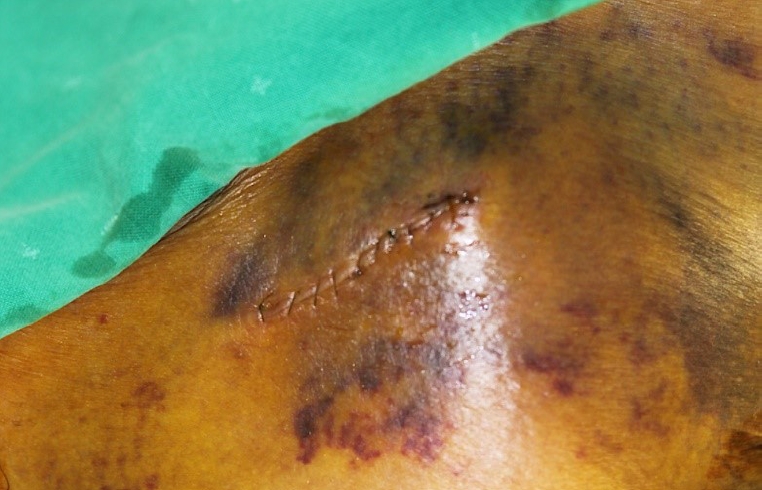
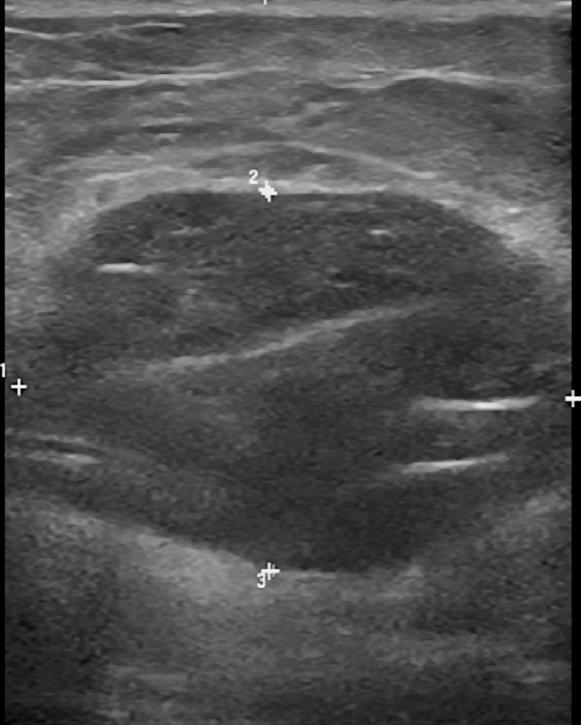
We referred to a recent opinion article that reported a 3-level grading system for pocket hematomas and performed aseptic aspiration after alcohol and povidone preparation on grade 2 and 3 hematomas (Fig. 1) that were highly likely to become infected (Table 1) [12]. In some cases, we used an ultrasound device to detect hematoma (Fig. 2) before performing aspiration, especially when the case was severe or when we were unsure why the wound was swelling. Such cases required more careful investigation and follow-up for hematoma.
We analyzed the number of patients with hematoma, treatment methods for hematoma (conservative, aspiration, or other surgical treatment), number of aspirations, total aspiration volume when performed, and the results of aspiration. For these patients, we also conducted a chart review of underlying diseases (congestive heart failure, renal failure, thrombocytopenia) that are known to increase the risk of pocket hematoma development [13,14]. We evaluated anticoagulant and antiplatelet therapy history before undergoing the CIED procedure to investigate their relationship. Furthermore, we also analyzed the frequency of pocket hematoma, according to age and CIED type, to investigate their relationship with pocket hematoma formation.
The study was approved by the Institutional Review Board of Wonkwang University Hospital (IRB No. 2021-07-013), and the patients provided written informed consent for the publication of this study and the use of their images.
Results
Among those included in the study, 80 patients (14%) presented with a pocket hematoma (Table 2). In our study, hematoma occurred more frequently in men than in women. Hematoma was more frequent in older adults, especially those in their 70s (Table 3). Furthermore, in descending order of frequency, the frequency of pocket hematoma by CIED type was ICD> PPM>CRT (Table 4). The incidence of pocket hematoma was 14.4% in the “De novo” group, and 11.4% in the “Replacement” group. In the “Replacement” group, those who underwent ICD replacement showed the highest frequency (25%) (Table 5). In descending order of frequency, the most common underlying diseases were hypertension, arrhythmia, chronic kidney disease, and congestive heart failure in patients with hematoma (Table 6). In this study, 5% of patients had underlying thrombocytopenia, which was defined as a platelet count of less than 100,000/µL. Patients with hematoma commonly presented with comorbidities. Among the 80 patients with pocket hematoma, only three patients did not have a significant medical history.
In our study, anticoagulant and antiplatelet therapies performed before admission were, in descending order of frequency, aspirin, clopidogrel, and vitamin K antagonists (Table 7). Among the 80 patients with hematoma, 52 received at least one perioperative anticoagulant and antiplatelet therapy, as against 35% of patients who did not receive any therapy (Table 8).
A total of 58 patients were treated with aspiration (Table 9), of which 52 cases were treated using aspiration only (no additional surgical procedure). The six remaining patients underwent aspiration with some type of surgical procedure. Of these patients, two underwent hematoma evacuation, Barovac insertion, and device repositioning with flap (rotation flap or latissimus dorsi flap) surgery to cover the defect of the wound after performing aspiration treatment. Three patients underwent only hematoma evacuation surgery after aspiration treatment, and one patient required only incision, hematoma rolling, and primary closure. Five patients in the surgical treatment group, whose wounds had been in poor condition since immediately after the CIED procedure, underwent hematoma evacuation, Barovac insertion, and abscess incision and drainage. There were 17 patients in the conservative treatment group. Patients treated with aspiration were divided into one to five aspiration attempts. Most commonly, the patients underwent one or two aspiration procedures (87.93%). Patients were grouped in terms of aspiration volume (volume ≤10 mL, >10 and ≤20 mL, >20 and ≤30 mL, >30 and ≤40 mL, 40 mL or higher). Most patients had an aspiration volume of ≤20 mL (74.13%). Of all the hematoma cases treated only with aspiration, 89.65% were treated without any complications (Table 10).
Discussion
The use of CIED has increased over the last decade due to diversifying indications and increasing life expectancy. One of the most common complications of the CIED procedure is the pocket hematoma, which can be small and may be managed conservatively [4,15]. In this study, we aimed to explore whether it would be possible to lower the risk of infection by aseptically removing the hematoma at an early stage through aspiration. We found that aseptic removal of hematoma by aspiration alone was effective in most patients. We noted a low complication rate, with complications that could not be attributed to the aspiration procedure. Only 10.34% of the patients had complications, i.e., cases where hematoma or pocket hematoma could not be treated with aspiration alone or cases where the condition exacerbated to infection, necessitating surgical intervention. Of the six patients who needed additional procedures to treat hematoma, one patient needed only incision, hematoma rolling, and primary closure. Three only required hematoma evacuation surgery because the hematoma size was not decreased by aspiration treatment alone. These patients did not present any symptoms of infection, and their hematoma was completely healed. Only two out of six patients in the complication group presented with severe infection symptoms, including uncontrolled pain with severe swelling, no reduction in bloody discharge through the incision site, rapid skin color change in the area where the device was inserted, and a continuous elevation of inflammatory markers such as erythrocyte sedimentation rate, C-reactive protein, and white blood cell counts soon after the CIED procedure. In these cases, infections were not caused by aspiration treatment. The two patients had hematoma evacuation surgery first because the condition of their wounds had worsened soon after the CIED procedure. Aspiration was only used in the postoperative period after evacuation surgery, suggesting that the infection was not caused by aspiration. Therefore, we can conclude that none of the 58 patients with hematoma treated using aspiration acquired the infection from the aspiration procedure.
Some studies have reported that pocket hematoma is more common among women than men and affects older adults more commonly [13,14,16]. Although our sample size was small, the hematoma was more common among men, contrary to previous reports. The results of the age-specific incidence rate, however, were in line with the findings of previous studies (i.e., higher incidence among older adults).
Patients receiving ICD or CRT implants were reportedly more likely to have pocket hematoma than those receiving permanent pacemakers [14]. Our results also aligned with these findings; in our study, the hematoma was more common among patients receiving ICD, with more patients having permanent pacemakers than CRT implants. It is known that device complexity and the number of leads were significantly associated with increased infection risk [17]. In one study, the infection risk was higher in implantable device replacement procedures than in first implants [18]. Also, patients with comorbidities such as congestive heart failure, renal failure, and thrombocytopenia have an increased risk of pocket hematoma formation [13,14].
Clinically significant pocket hematoma is associated with a higher risk of device infection, which is reportedly associated with a mortality rate of 0% to 18% [6-8,19,20]. There are several possible mechanisms of hematoma development that predispose patients to CIED infection. Some of these are: (1) postoperative contamination caused by tension from hematoma, which causes a breach in the wound, and (2) pressure from the hematoma may cause pressure-induced tissue necrosis and decrease the ability of local tissue to fight infection [21,22]. These conditions eventually create fertile ground for sustained microbial colonization.
Currently, there is no specific treatment for pocket hematomas in the immediate term, except for conservative treatment such as compression dressings [4,15]. Preventing pocket hematoma formation is challenging because patients who undergo CIED implantation or replacement are often on anticoagulation and antiplatelet therapy due to associated comorbidities [2]. As a result, current measures primarily focus on pre-operative strategies to reduce hematoma formation. For example, in terms of anticoagulant and antiplatelet therapy, withholding warfarin for 2–3 days before implantation in patients at low risk of thromboembolism can reduce the risk of pocket hematoma [23]. However, in patients with moderate-to-high risk of thromboembolism, oral anticoagulants should be continued to avoid a situation requiring bridging therapy during the CIEDs procedure [23]. In recent meta-analyses, the continuation of warfarin was reported as the best strategy for moderate-tohigh-risk of thromboembolism in patients to reduce pocket hematoma formation [24]. Concomitant use of antiplatelet agents in patients undergoing device surgery doubles the risk of clinically significant hematoma. In our study, the patients’ intake of antiplatelet and anticoagulant medications was either interrupted or uninterrupted, depending on their condition. If a patient was at risk of pocket hematoma, the medication was discontinued before and after the CIED procedure. Consequently, even if a patient consumed the medication for the procedure before admission, interrupting the medication intake would decrease the final effect, thereby reducing the probability of hematoma formation among patients consuming anticoagulant and antiplatelet medications. This is evident from the higher-than-expected rate of pocket hematoma formation in the patients who did not receive any antiplatelet and anticoagulant therapy. Clinicians have also focused on optimizing the procedure itself to reduce the risk of hematoma formation. Such efforts include subcutaneous insertion of CIED (not in the subpectoral area) [5], irrigation of the pocket, meticulous cauterization of all bleeding arteries, and use of absorbable hemostat (D-Stat Flowable Hemostat) [25].
Our study focused on exploring aspiration as the primary treatment method for pocket hematoma. This is contrary to the common understanding wherein aspiration is not recommended as a treatment for pocket hematoma due to the increased infection rate [6,9]. We found that aspiration was an effective method for hematoma treatment and caused no complications. Previous studies did not specify the specialty of the surgeon who performed aspiration as well as the procedure used for aspiration. In our study, the aspiration procedure was performed by plastic surgeons familiar with the procedure and surgery, and the patients were followed up by plastic surgeons who were trained as specialists in applying dressings. Furthermore, the procedure and post-dressing treatment after aspiration were not complex. Aspiration was not performed in an operating room; instead, it was performed aseptically in a private room for hospitalized patients and in our plastic surgery room for outpatients. Successful aspiration without any complications in this study further supports the feasibility of aspiration as an effective treatment for pocket hematoma. Our findings suggest that the procedure can be safely performed aseptically using alcohol and povidone preparation and aseptic gloves, taking care to avoid contact between the aspiration needle and the CIED implant. We also recommend using an ultrasound-guided aspiration for clinicians unfamiliar with the procedure.
One of the strengths of this study is that, since January 2011, the patients were followed up by both cardiologists and plastic surgeons in our hospital from the beginning of the CIED procedure to the resolution of pocket hematoma. This allowed us to capture high-quality data during the follow-up period. However, there were several limitations to our study. First, the patients were subject to anticoagulant and antiplatelet treatment, depending on each patient’s condition, meaning that analysis of the actual effect of medication on pocket hematoma formation would have been impacted. Second, medical records and data were focused on patients with grade 2 or 3 pocket hematoma, for which aspiration therapy could be used. Consequently, a number of patients who received conservative treatment for grade 1 hematoma were missed, making the ratio of the conservative treatment patient group slightly lower than the actual figure.
In conclusion, clinicians must place much emphasis on reducing the risk of pocket hematoma formation, considering the high mortality rates and complications in the other studies mentioned above. Moreover, when planning a CIED procedure for patients with congestive heart failure, renal failure, and thrombocytopenia, which reportedly increase the risk of hematoma development, the CIED procedure must be carefully and meticulously planned, examining the risks and benefits.
While pocket hematoma formation could not be prevented despite knowledge of the risk factors from previous reports, we aimed to treat hematoma and to prevent it from aggravating to CIED infection. Our study confirmed that aspiration could be an effective treatment method for pocket hematoma.