Penile Distortion Caused by a Large Epidermal Cyst after Augmentation Penoplasty: A Case Report
Article information

Abstract
Although an epidermal cyst is a common cutaneous lesion that can present anywhere on the body, it is not easily found on the penis. A 64-year-old man visited Hanyang University Guri Hospital with a soft, large, subcutaneous mass on the right ventral side of the penile shaft that caused distortion. He had augmentation penoplasty 20 years ago with a dermal fat graft, but had not experienced any asymmetry or infection of the penis during the postoperative period. Three years prior the patient had observed a lump on his penis that had since grown slowly, causing distortion of the penis and sexual dysfunction. The mass was excised and diagnosed by a pathologist as an epidermal cyst. The patient was satisfied with the aesthetic result, and his sexual function gradually returned. Here, we introduce an extremely rare case of a penile epidermal cyst causing penile distortion. We suggest that the cause for its formation was incomplete de-epithelization of the graft during dermal fat grafting.
Introduction
Epidermal cysts, also called epidermal inclusion cysts, are one of the most common benign lesions and can be found on practically all regions of the body. Nevertheless, penile epidermal cysts are relatively rare [1,2]. Epidermal cysts of congenital origin, which are usually caused by abnormal embryologic closure of the median raphe, are easily discovered by parents [1]. Lesions seen in adults are mostly caused by trauma or are sequelae of complications after surgery; lack of symptoms such as discomfort often result in late detection. If epithelium remains enclosed during wound healing after trauma or surgery, keratinization occurs and leads to cyst formation [3]. While epidermal cysts can be evaluated by sonography, computed tomography (CT), or magnetic resonance imaging (MRI), definitive diagnosis is based on microscopic analysis of the excised biopsy specimen. This report presents an extremely rare case of a large epidermal cyst causing penile distortion that occurred years after augmentation penoplasty with dermal fat graft. Written informed consent from the patient for the publication and use of photographs and radiologic images was obtained.
Case
A 64-year-old male patient presented with a soft, cystic, large subcutaneous mass on the right ventral side of the penis, located in the distal half of the penile shaft, causing distortion, with no underlying disease. The mass was about 5 cm in diameter and was soft and non-tender. It did not decrease in volume when pressed, and was mobile against the base and more so against the skin envelope. Twenty years earlier the patient had undergone augmentation penoplasty with dermal fat graft at a clinic, the graft being harvested from the left gluteal fold. The dermal fat graft was inset through a vertical incision on the dorsum of the penis. The patient had not experienced any asymmetry or infection of the penis in the past postoperative period. However, the patient had noticed a lump on his penis 3 years prior to his present presentation. The initial small mass had not caused any symptoms. However, as the mass grew gradually, the patient suffered from sexual dysfunction including painful erection and difficulty with sexual intercourse. There were no signs of infection or inflammation such as redness or additional swelling (Fig. 1). Preoperative inflammatory values of white blood cell count and C-reactive protein level were found to be normal at 8,500/µL and 0.1 mg/dL, respectively.

Preoperative photograph. The mass distorting the penis showed no signs of infection, but caused difficulty with erection and sexual intercourse.
To evaluate the penile mass, MRI was performed. A T2-weighted MRI showed a 40×40×47 mm benign-looking, en-capsulated cystic mass with a uniformly enhancing cyst wall (Fig. 2). The contents of the mass showed relatively uniform intensity. The mass was exerting pressure, producing a bend in the penile shaft, but was located on the Buck's fascia with no infiltration, and the boundary with the corpus cavernosum and corpus spongiosum was clearly defined.
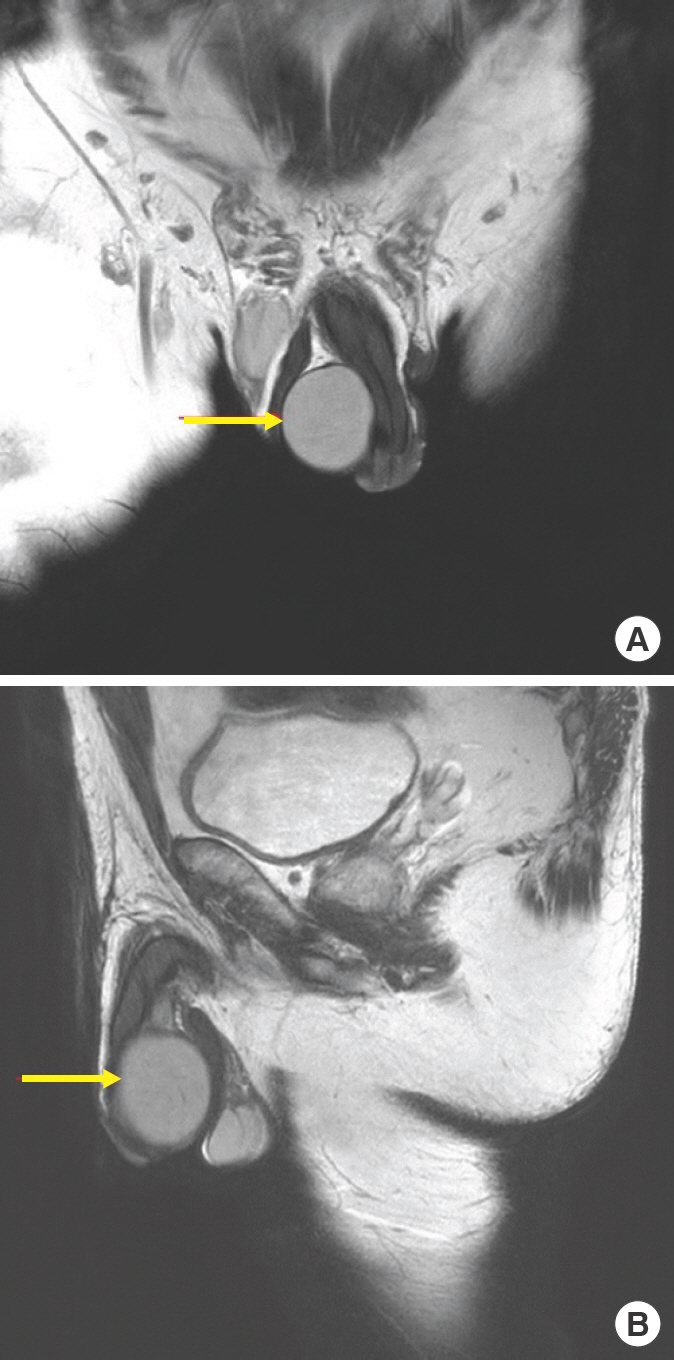
Preoperative magnetic resonance imaging of the penile mass. (A) Coronal view. The mass (arrow) has a well-defined boundary with the corpus cavernosum, corpus spongiosum, and scrotum. (B) Sagittal view. The mass (arrow) is distorting the penis due to compression.
Complete excision and biopsy were performed under general anesthesia. Remnants of the grafted dermal fat were not observed (Fig. 3A and B). Whitish necrotic material was found after bisection of the mass (Fig. 3C). Pathohistological examination of the mass revealed a cyst wall including stratified squamous epithelium and a granular layer containing epitheli-al detritus including abundant keratin flakes and cholesterol clefts.
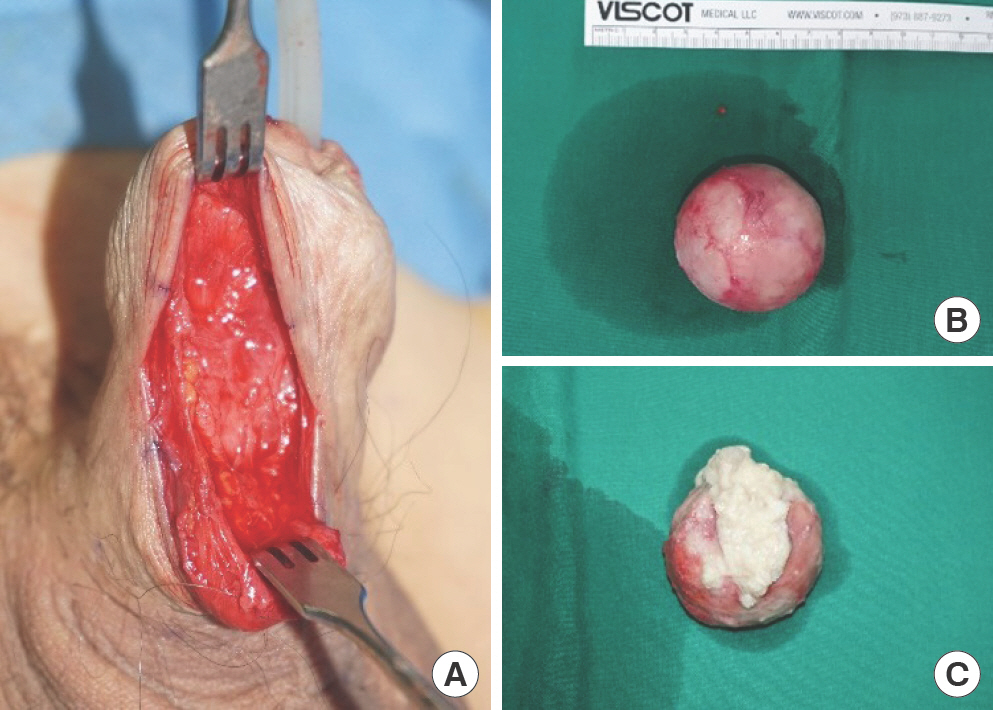
Intraoperative photographs during mass excision. (A) Mass excised from the penile shaft. The mass was clearly de-marcated, and no remnants of grafted dermal fat were seen. (B) Excised mass measuring 5 cm in diameter. (C) Transected mass: the cystic wall surrounded a whitish necrotic material.
After mass removal, the penile distortion was resolved with-out complications. The patient was satisfied with the aesthetic result, and his sexual function gradually returned. Two months after the excision, the penile incision site scar was minimal and the penile shaft was straightened, while the patient did not complain of any consistent symptoms (Fig. 4). No complications occurred through the 6 months’ follow-up.
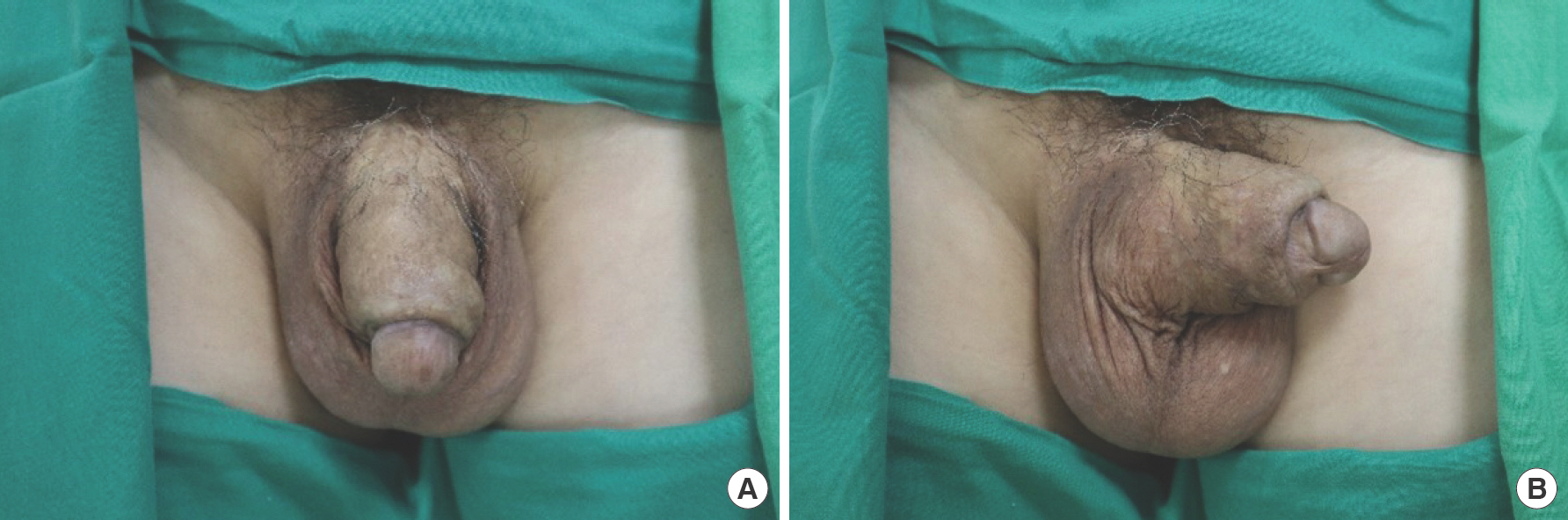
Postoperative follow-up photographs after 2 months. (A) The penile shaft was straightened after cyst excision. (B) Only minimal scarring is observed and the patient was satisfied.
Discussion
While epidermal cysts are one of the most common benign tumors and can occur anywhere in the body, epidermal cysts in the penis are rare. Penile epidermal cysts can be classified into congenital cysts and secondary cysts caused by previous trauma or operation [2]. Congenital cysts in children are also called median raphe cysts, as they usually generate from abnormal embryologic closure within the median raphe and can develop anywhere along the ventral side midline of the male urogenital region, between the urethral meatus and the anus [3,4]. Secondary cysts may occur from occlusion of hair folli-cles, mechanical implantation of grafts and injections, or obstruction of eccrine ducts.
Most epidermal cysts are usually small in size, soft, fairly mobile instead of being firmly adhered to a base structure, and solitary, but some cases are multifocal [5]. They are usually as-ymptomatic, but as they grow in size over time, they may cause symptoms due to infection or trauma. Penile epidermal cysts can compress the urethra, causing voiding difficulty, uri-nary tract infection, and pain in sexual intercourse due to penile distortion [6,7].
In earlier literature, ultrasonography or CT scan with careful examination was recommended for diagnosing penile epidermal cysts [8]. More recently, MRI is considered the most use-ful tool for delineation of anatomical boundaries [6]. In this study, MRI was used as a diagnostic tool, clearly establishing the boundary between the epidermal cyst and the corpus cavernosum or corpus spongiosum.
Most masses occurring on the penis need to be removed surgically. Complete excision is recommended when the cyst is fairly large and shows growth tendency or risk of anatomical problems with urethral obstruction or sexual intercourse. Complete removal of the cyst and careful follow-up are considered the treatment of choice [8]. Aspiration or simple drainage result in a very high recurrence rate, also requiring continuous excision [6].
As a man's perception of his penis has a significant effect on sexual identity and self-esteem, some male patients undergo aesthetic genital surgery to change the appearance of the penis or scrotum [9]. Therefore, various options for penile augmentation have been developed, including surgical methods such as lipoplasty, suspensory ligament release, flaps, or grafting, in addition to nonsurgical methods of injecting silicone, fat, and fillers [10–12]. After penile augmentation, major complications such as wound dehiscence, infection, hematoma, adhesion, and glans numbness and minor complications such as paradoxical shortening due to adhesion and erectile malfunction can be observed. Rare complications such as foreign body reactions and epidermal cyst formation due to implantation of epithelium after incomplete de-epithelization have been re-ported after injection, implantation, and grafting [10,13,14].
In our case, the patient had undergone augmentation penoplasty through a dermal fat graft 20 years prior to his visit. Dermal fat graft for penile girth enhancement is classically performed with partial circumcision or transverse pubic incision and increases the penis about 2 to 4 cm in circumference. In general, the dermal fat graft is processed to be suitable for inset through de-epithelization, and then fixed to Buck's fascia using absorbable sutures [9,12]. As our patient's surgery was performed by an outside surgeon 20 years ago, it is presumed that a vertical pubic incision was selected as the appropriate option at the time. Although the exact size of the graft performed at that time is not known, it seems that the graft was sufficiently wrapped around the circumference at the time of surgery considering the current shape. Since the patient did not feel any discomfort immediately after surgery, it is as-sumed that there was no early complication like seroma or hematoma.
However, as the penile mass had grown on the layer in which the dermal fat graft was set, it was suspected that the cause of epidermal cyst development was mechanical implantation due to remnants after incomplete de-epithelization of the dermal graft. After cyst removal, the symptoms were resolved, and no problems were noted during the 6 months fol-low-up period; as the recurrence rate is significantly lowered when proper removal was done, we expect little possibility of recurrence or other late complications.
To the best of our knowledge, few publications have report-ed epidermal cyst formation after augmentation penoplasty. Moreover, reports on large epidermal cysts that impede sexual activity are even rarer [15]. Presenting a rare case of penile epidermal cyst after augmentation penoplasty, we stress that pre-cise de-epithelization is crucial to avoid surgical wound complications such as epidermal cyst formation. We believe that this case study will be helpful in further understanding augmentation penoplasty using dermal fat grafts and postoperative epidermal cyst development.
Notes
No potential conflict of interest relevant to this article was reported.