Pyoderma Gangrenosum Overlying Venous Insufficiency: An Inevitable Misdiagnosis
Article information

Abstract
Pyoderma gangrenosum (PG) is a destructive inflammatory disease characterized by painful ulcerative lesions with neutrophilic infiltration in the dermis. Although the etiology and pathogenesis are poorly understood, uncontrolled inflammatory responses to nonspecific stimuli may trigger the development of PG. Here, we report a rare case of PG arising above a venous insufficiency lesion. The most typical diagnosis for an ulcer at such a location is venous ulcer. However, our atypical case of PG emphasizes that PG can be induced by ischemic conditions, such as venous insufficiency. Debridement and skin grafting, which were performed based on an incorrect diagnosis, worsened the PG lesion and provoked a severe pathergy phenomenon. Thus, surgeons should consider PG in the differential diagnosis of intractable venous ulcers in order to ensure an accurate diagnosis and prompt treatment.
Introduction
Pyoderma gangrenosum (PG) is a destructive inflammatory disease characterized by painful ulcerative lesions with neutrophilic infiltration of the dermis. The etiology and pathogenesis of PG are poorly understood [1]. The pathergy phenomenon, a hallmark of PG, is a condition in which trivial trauma leads to the development of similar lesions that may be resistant to healing [2]. This phenomenon implies that uncontrolled inflammatory responses to nonspecific stimuli may trigger PG [3]. Approximately 50% of PG cases have been associated with a wide variety of disorders, including inflammatory bowel disease and other hematologic and rheumatologic diseases [4]. However, few cases of PG have developed after only minor trauma with ischemia [5,6]. Herein, we presented the case of 66-year-old man, who developed PG masquerading intractable venous ulcers. The written informed consent was obtained from the patient.
Case
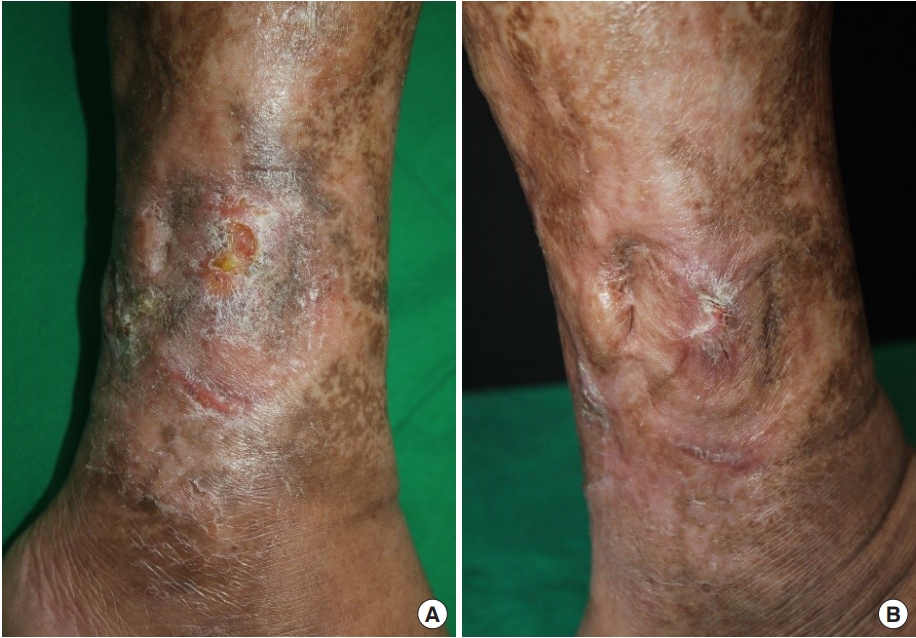
A 66-year-old man was referred to Chung-Ang University Hospital and presented with multiple painful ulcers on both lower legs. These ulcers had been recurrent over the past 4 years. A year before the ulcers arose, he had undergone a total knee replacement surgery (TKR) for degenerative osteoarthritis. The ulcers were well circumscribed, with purplish elevated borders, and their granulomatous bases were covered with yellow fibrinous tissue. Pitting edema surrounded by a brown, reticular pigmented patch was also identified (Fig. 1). Before being referred to our clinic, he had been diagnosed with a venous leg ulcer based on clinical appearance and history of TKR, and he was treated with conventional therapy, including leg elevation, wound dressing, oral anticoagulants, antibiotics, and five split-thickness skin grafts. Despite the prolonged treatment of the venous leg ulcers, clinical improvement was not observed, and new lesions developed at the skin graft donor and recipient sites. These new lesions on donor sites demonstrated a pathergy phenomenon. For further evaluation, an immunological assessment was carried out: the presence of anti-cardiolipin antibody, rheumatoid factor, lupus anticoagulant, anti-double-stranded DNA antibody, anti-Ro/SS-A, and anti-La/SS-B was tested. The results of these tests were negative. A biopsy from the center of the lesion revealed diffuse neutrophilic infiltration in the necrotic upper dermis and neutrophil-predominant perivascular infiltration with minimal vascular damage. We did not find any fibrinous deposits or intravascular thrombosis (Fig. 2). Because of the combination of certain characteristics, such as pathergy and neutrophilic infiltrates on biopsy, a final diagnosis of PG was made after excluding other diseases such as malignancy and infections. Therefore, treatment with high-dose systemic corticosteroids (45 mg/day) was initiated along with conventional treatment for venous ulcers, including leg elevation and dressing changes. During the follow-up period, the lesion resolved dramatically, and his pain rapidly diminished (Fig. 3).

Multiple necrotic ulcers with purplish, elevated borders. (A, B) Leg edema surrounded by a brownish, reticular pigmented patch was also present.

Biopsy of the ulcer. (A) Diffuse neutrophilic infiltration in the necrotic upper dermis (H&E stain, ×100). (B) Neutrophil-predominant perivascular infiltration with minimal vascular damage (H&E stain, ×400).
Results after the treatment. (A) Two months and (B) 4 months after steroidal treatment.
Discussion
The mechanisms and pathophysiology of PG are elusive and likely multifactorial. An accepted and validated diagnostic criterion for PG is still lacking [7]. An anomalous autoimmune or inflammatory response is believed to be the main component of PG’s pathophysiology [8], and this is supported by the efficacy of immunosuppression with systemic steroids and cyclosporine in treating PG. Furthermore, inflammatory and autoimmune responses are exacerbated in ischemic conditions such as venous insufficiency [9].
Su et al. [10] proposed diagnostic criteria for PG as fulfilling two of major criteria and two of minor criteria of the following. Major criteria: rapid progression of a painful, necrolytic cutaneous ulcer with an irregular, violaceous border, and exclusion of other causes of cutaneous ulceration. Minor criteria: history suggestive of pathergy or clinical finding of cribriform scarring, systemic diseases associated with PG, compatible histopathological findings and response to treatment. In our case, though three of the minor criteria was fulfilled except for having systemic diseases, major criteria was not fulfilled at first for excluding other causes of ulceration was not possible because of the chronic venous ulcer patient had previously. In addition, Koo et al. [11] suggested some of the characteristics that could differentiate PG from chronic venous ulcer. While chronic venous ulcer usually affect only legs, PG could appear on different parts of the body and also is usually associated with systemic diseases and pathergy with distinct features of pustules, purulent discharge, undermined borders, and crater-like holes. However, in our case, ulceration only appeared on legs and did not seem to present the features that differentiated PG from venous ulcer.
We found our case fascinating because the lesion did not quite show known characteristics of PG and plus was superimposed over a site of venous insufficiency, confusing clinicians and leading to an inevitable misdiagnosis of venous ulcers, thus delaying appropriate treatment. The debridement and skin grafting, which were performed based on an incorrect diagnosis, worsened the PG lesion and provoked a severe pathergy phenomenon. This led us into immunological assessments and skin biopsy to rule out other possible diseases and concluded with an elusive PG and properly treat the patient.
In conclusion, to avoid misdiagnosis, a skin biopsy should be considered when a venous leg ulcer is resistant to healing with conventional ulcer treatments. Like in our case, though the featuring characteristics of the lesion may not let clinicians suspect a disease, biopsy could be a key step in diagnosing a hard case. Biopsies are useful, not only in diagnosis of PG, but also in excluding other diseases such as malignancy and infections [12]. Taking variety of diagnosing tools into consideration for chronic wounds will not just save time, but will have a major effect on the outcome of the treatment.
Notes
No potential conflicts of interest relevant to this article are reported.