









Introduction
Extensive degloving injury that involves severe damage to the osteocutaneous and neurovascular systems is usually caused by rolling machines or wheels, and the lower extremities are a common site of such injuries. These injuries can cause serious complications, such as hematoma or wound infection, sepsis, and even death [1].
Degloving injuries over the entire lower extremities are particularly difficult to manage. Because protein loss and bacterial proliferation rapidly progress in the degloved wound, it is important to regain tissue coverage as early as possible. Though temporary coverage (such as cadaver skin coverage or biological dressings) may prevent protein loss and bacterial proliferation, such injuries ultimately require autologous grafts for complete recovery. Meanwhile, due to extensive damage to the lower extremities including the thighs, there already are constraints to the range of available skin graft donor sites, and the recipient bed condition is often too poor to directly sustain grafts. Recycling and use of the degloved skin can be attempted, but there have been reports of the injured region worsening due to infection [1]. Therefore, an effective strategy for treating an entire degloving injury is required. In this article, by assessing the clinical course and therapeutic outcomes of patients, we introduce a treatment strategy for entire lower extremity degloving injury.
Case
This study was a retrospective review of medical records from March 2018 to April 2021. Following institutional guidelines, this study was approved by the Institutional Review Board of Dankook University Hospital (IRB No. 2022-02-004). The informed consent was waived. Of the total of 10 patients who had lower extremity degloving injury during the study period, three patients had injuries encompassing their entire extremity. We analyzed the age, sex, past medical history, cause of trauma, trauma injury severity score (TRISS), combined injuries including fractures, comorbidities, frequency of operations, and duration of hospitalization. The patient's age, mode of injury, and both anatomical and physiological degrees of injury severity were required to determine the TRISS probability of survival. Additionally, the level of C-reactive protein (CRP) was checked as an inflammatory marker. The following treatment outcomes were evaluated: post-discharge progress, disability including range of motion, and psychiatric problems. In the course of treatment, the following strategy was taken.
Treatment strategy (Fig. 1)
Fig. 1.
A schematic image for the treatment strategy. ICU, intensive care unit; IV, intravenous; ADM, acellular dermal matrix; NPWT, negative pressure wound therapy.
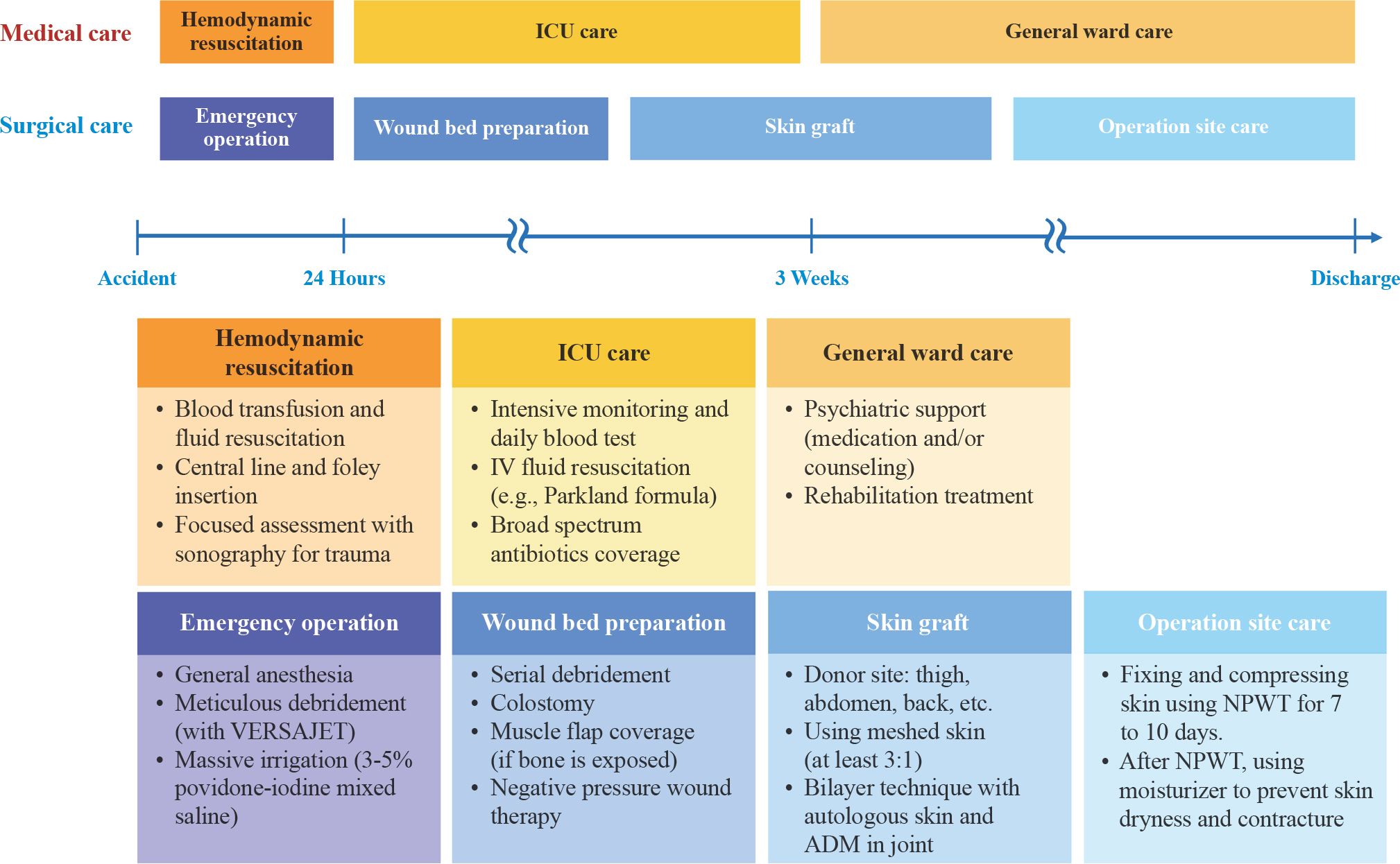
Initial treatment (within 24 hours)
Emergency surgery under general anesthesia should be performed as soon as possible, within 24 hours after trauma, before the maximum inflammatory response. At this time, all foreign bodies should be thoroughly removed, and the degloved skin should be extensively excised until there is fresh subcutaneous bleeding. A hydrosurgical tool (Versajet; Smith & Nephew Medical, London, UK) was the tool of choice for wound bed debridement. Massive irrigation should be conducted with at least 10 L of a suitable solution. For this study, we used a mixed solution of approximately 3% to 5% povi-done-iodine with saline.
Intensive medical care and wound bed preparation for skin graft (until 2–3 weeks)
After the initial treatment, intensive care is recommended for 2–3 weeks. During this period, (1) vital signs should be monitored hourly and daily blood tests should be performed to determine whether there is a septic condition. (2) Intravenous fluid resuscitation should be administered in accordance with burn treatment protocols (e.g., Parkland formula). (3) Simultaneously, antibiotics with broadspectrum coverage should be used. We started with carbapenem and vancomycin. Our antibiotic of choice was changed after a weekly wound swab culture. (4) Foley catheter insertion and prophylactic colostomy were also helpful because the degloved lower extremity wounds are usually located near the anus and urethra. (5) For preparing the wound bed, application of negative pressure wound therapy (NPWT) is recommended as soon as possible after tissue necrosis has resolved. We administered NPWT three times per week with the patients under general anesthesia. Meanwhile, muscle flaps may be useful for covering deeply depressed tissue defects or exposed bones.
Skin graft (within 3 weeks)
It is recommended that the skin graft be performed in less than 3 weeks before biofilm formation. Considering the difficulty of obtaining donor sites, the skin should be harvested carefully. We mostly harvested the skin on the opposite leg, abdomen, back, and both buttocks. Additionally, we always applied a meshed graft (at least a 3:1 mesh ratio) to cover as wide an area as possible. We used a bilayer technique with meshed autologous skin and an acellular dermal matrix (ADM; Matriderm, Dr. Suwelack Skin and Health Care AG, Billerbeck, Germany) around joints to prevent contracture. NPWT was then applied for 7–10 days. The skin graft procedure usually involves several operations.
Case presentation
A total of three female patients with no underlying diseases were included, with an average age of 58.0±15.7 years (range, 44–75 years). One patient had a motor vehicle accident, and the other two patients had pedestrian accidents. The average survival probability was 85.3%±11.4% (range, 75.6%–97.8%) according to the TRISS. The average injured body surface area was 20.3% (range, 18.0%–22.5%). All patients had open fractures, meaning the orthopedic department was involved in the treatment. The average total length of hospital stay was 227.7±74.8 days (range, 181–314 days), and the average intensive care unit (ICU) stay was 36.7±30.2 days (range, 11–70 days). Patients required an average of 40.3±8.6 (range, 31–48) surgeries. Cases 1 and 2 required one flap coverage each. In case 1, a gastrocnemius muscle flap was used to cover the exposed fibular bone area. In case 2, an anterior thigh deep defect was filled using the rectus femoris muscle. The average number of skin grafts was 3.7±1.2 (range, 3–5), and that of amputations was 1.3±2.3 (range, 0–4). Additionally, the average number of other procedures done in the operating room, including cleansing, meticulous surgical debridement, antiseptic dressing or NPWT, was 34.7±5.8 (range, 28–38) (Table 1). NPWT could not be used immediately after the initial surgical debridement. Nevertheless, the goal was to apply NPWT as soon as feasible once bleeding subsided. After the initial surgical debridement, NPWT was applied on an average of 9 days later. When NPWT was applied, we used a DACC (dialkylcar-bamoyl chloride)-coated dressing material (Sorbact Compress; Abigo Medical AB, Askim, Sweden) as a contact layer between the wound bed and the polyurethane sponge foam. The average CRP level was the highest on day 3 after the injury, and sharply declined up to day 14.3. CRP levels fluctuated, recording a second decline on day 35.3 (Fig. 2). After treatment, all patients suffered from post-traumatic stress disorder (PTSD). On joint disability evaluation, the range of motion was limited in all cases, but improved with rehabilitation (Table 2, Supplementary Video 1). Detailed characteristics were explored for each case.
Table 1.
Characteristics of three patients
| Characteristics | Case 1 | Case 2 | Case 3 | Mean±SD |
|---|---|---|---|---|
| Age (yr) | 44 | 75 | 55 | 58.0±15.7 |
| Sex | Female | Female | Female | |
| Past medical history | None | None | None | |
| Cause of trauma | Motorcycle TA (bus crash) | Pedestrian TA (by bus) | Pedestrian TA (by fork lift) | |
| Survival probability (%) a) | 97.8 | 75.6 | 82.5 | 85.3±11.4 |
| Trauma region (TBSA, %) | Left inguinal to toe (18.0) | Right inguinal to ankle and left knee to ankle (22.5) | Left lower abdomen to ankle (22.0) | |
| Combined injury | Left toe, ankle and fibular fracture | Left ankle and pelvic fracture | Pelvic fracture and rectovaginal fistula | |
| Total LOS (day) | 314 | 181 | 188 | 227.7±74.8 |
| ICU LOS (day) | 11 | 70 | 29 | 36.7±30.2 |
| Total no. of operation | 48 | 42 | 31 | 40.3±8.6 |
| Flap coverage | 1 | 1 | 0 | 0.7±0.6 |
| Skin graft | 5 | 3 | 3 | 3.7±1.2 |
| Amputation | 4 | 0 | 0 | 1.3±2.3 |
| Etc. b) | 38 | 38 | 28 | 34.7±5.8 |
| Anesthesia type | ||||
| General | 19 | 19 | 19 | 19.0±0.0 |
| Spinal | 1 | 0 | 0 | 0.3±0.6 |
| Local | 28 | 23 | 12 | 21.0±8.2 |
| Discharge disposition | Home | Home | Home |
Fig. 2.
Graph of three patients’ C-reactive protein (CRP) levels during hospitalization. CRP levels peaked at 3 days on average and declined below 10 mg/dL at 15 days. CRP levels were usually stable after 4 weeks.

Table 2.
Post-treatment sequelae and complications
Case 1
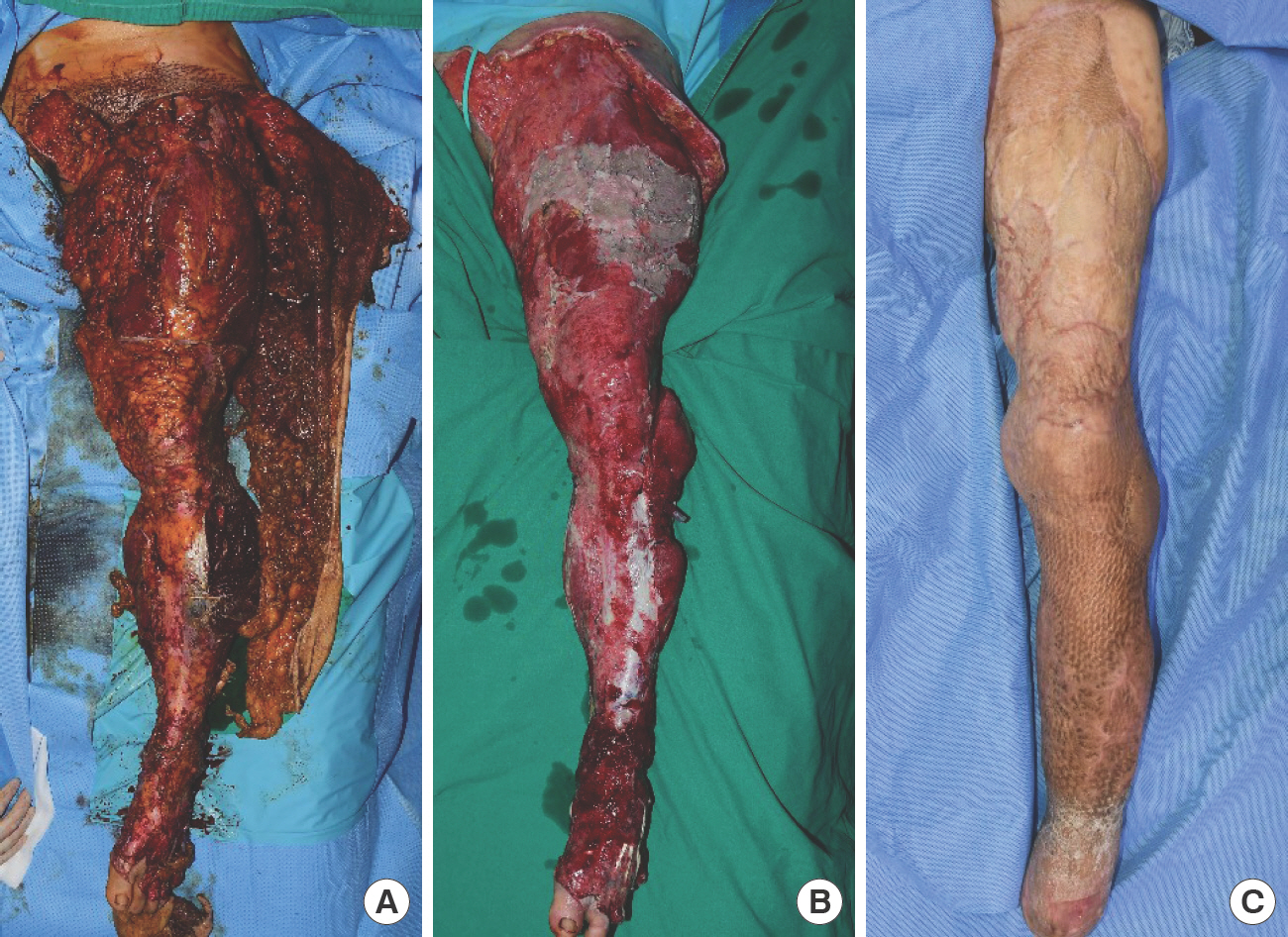
The injury involved the 3rd to 5th toes and ankle, and was accompanied by open fracture with necrosis which started from the distal area, for which serial amputations were performed. The third and fourth toes were initially amputated at the meta-tarsal-phalangeal joint level; as necrosis progressed, a Lisfranc amputation was performed. An orthopedic surgeon was consulted for lower extremity and pelvic bone fractures, and conservative therapy was performed. After wound management was completed, it was difficult for the patient to stand with both feet due to ankle plantar flexion. However, rehabilitation helped the patient reach 80° of knee flexion and ambulate using crutches (Fig. 3).
Case 2
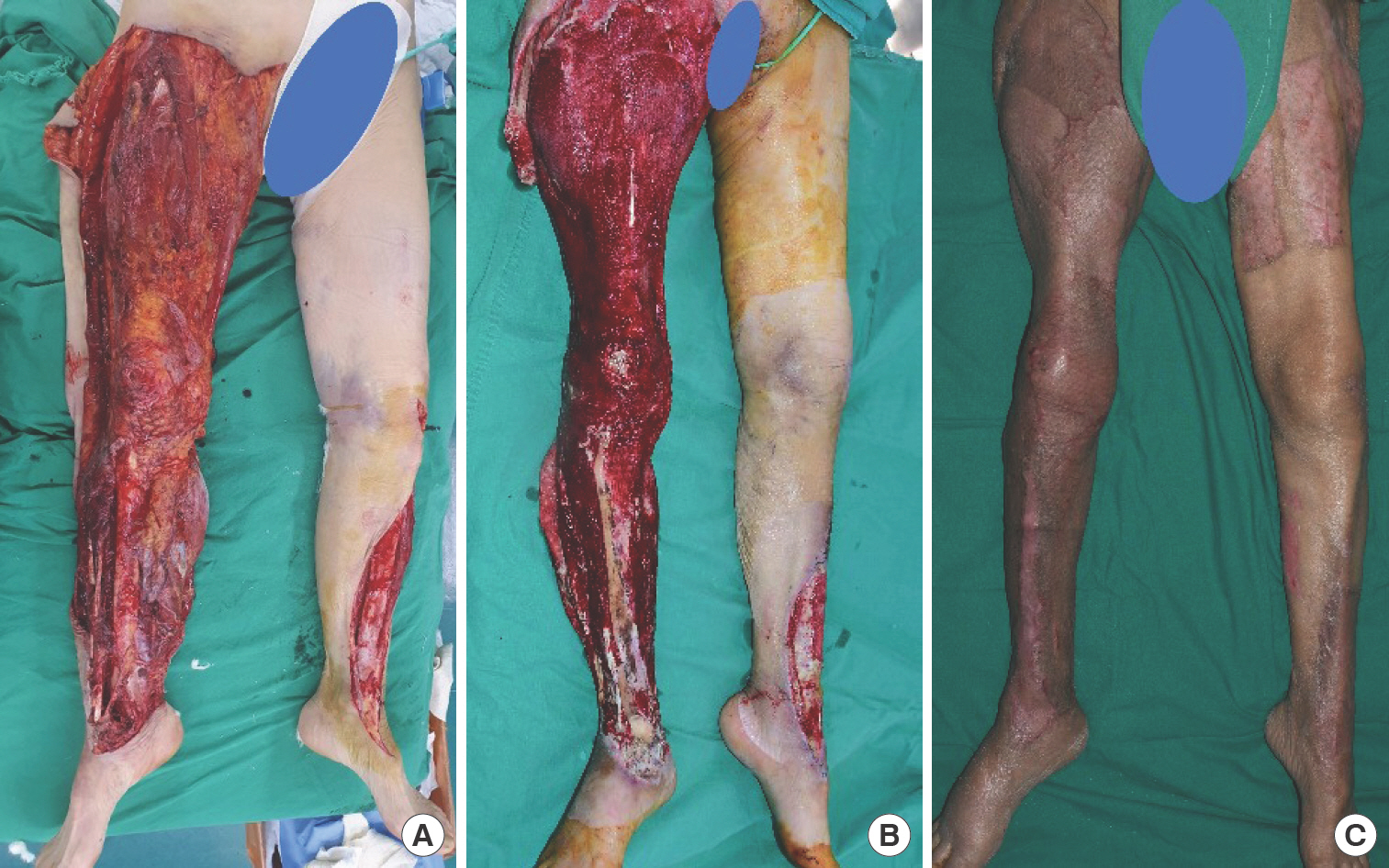
This was the oldest patient and had the lowest survival probability (75.6%) among the participants. The patient had injuries on both legs, from the inguinal region to the ankle on the right side and from the knee to the ankle on the left side. A pelvic bone fracture was treated conservatively after consulting an orthopedic surgeon. A calcaneustalus-tibia axial spin fixation was performed and maintained for 2 weeks to stabilize the ankle. These fractures and treatments did not significantly obstruct degloving wound management. The patient had the longest stay in the ICU (70 days). Additionally, due to general weakness associated with advanced age, it was difficult for the patient to complete ambulation therapy. Thus, unlike other patients, crutch gait was impossible; the patient could only achieve wheelchair ambulation (Fig. 4).
Case 3
The patient had a degloving wound that had extended to the abdomen, as well as an open pelvic fracture. After consulting an orthopedic surgeon, the pelvic fracture was treated conservatively. As a result, her pelvic range of motion was limited compared with that of the other patients (80° of flexion and −15° of extension) (Fig. 5).

Discussion
Entire lower extremity degloving injuries are very serious and potentially limb-threatening soft tissue lesions that have a high risk of infection, which can cause life-threatening complications. Although several studies have demonstrated therapeutic methods for reconstruction, few studies have examined the clinical course of patients in a time sequence [1,2]. The primary concern for saving lives in cases of extensive degloved injuries is dealing with acute bleeding and hemodynamic instability. Furthermore, such injuries can cause protein and electrolyte loss, whose imbalances are associated with an increased risk of morbidity and mortality [3]. Meanwhile, additional fluid loss has been reported when NPWT is used in extensive wounds [4]. On the other hand, excessive volume repletion can result in pulmonary edema or renal failure; both are life-threatening. Therefore, it is critical to closely monitor the patient's fluid balance and body weight and adjust the fluid treatment accordingly. In the cases of this study, excessive fluid resuscitation was not performed beyond the fluid amount calculated using the Parkland formula. Also, electrolyte and hemodynamic status should be monitored daily to help guide corrective measures. Additionally, wound infection may result in sepsis, which requires both medical and surgical strategies. It is important to perform meticulous surgical debridement to reduce the risk of infection and critical colonization. Simultaneously, broadspectrum antibiotics that cover both gram-positive and gram-negative pathogens have been recommended [5]. In our cases, we started a combination therapy of carbapenem and vancomycin. We did not follow a typical regimen. Owing to loss of skin integrity, the need for long periods of invasive or-gan support, and a degree of functional immunosuppression in the ICU, patients with large degloving wounds are extremely susceptible to nosocomial infection. A combination of cephalosporin and aminoglycoside is typically advised as an empirical antibiotic [6]. However, with increasing use of antibiotics, there has been more development of resistant bacteria [7]. Use of such antibiotics is likely to promote the growth of resistant bacteria; therefore, we used them carefully, and if there was no reason to continue using them once the sensitivity data were obtained, we changed to other antibiotics. This underscores the need to review initial usage of antibiotics.
Pain management is an important consideration in injury recovery. Patients experience extreme pain due to the wide and exposed wound. After the trauma, surgical debridement or NPWT was performed two to three times a week until the skin graft was carried out. Though not sufficiently supported by research or clinical evidence, it is believed that general anesthesia at 2 to 3-day intervals may worsen the patient's general condition. Each patient's general condition was closely monitored and discussed with the anesthesiologist before each operation, and general anesthesia was administered for about 2 to 3 weeks to control the patient's pain. When the skin was covered to some extent and the patient could tolerate the pain, the procedures were performed without general anesthesia. In addition to intraoperative anesthesia, pain was controlled by a patient-controlled analgesia device (fentanyl plus meperidine) in the ward.
Ambulation is an important treatment outcome factor in entire lower extremity degloving injuries that directly affects the patient's quality of life [8]. Because entire lower extremity degloving injuries often extend from the toes to the pelvic joints, recovery of range of motion in joints to the extent that walking is possible is a challenge. Although the ideal treatment for ambulation is flap coverage, the use of free microvascular flaps has been limited due to altered peripheral hemodynamics, damaged recipient vessels, and donor site morbidity [9]. In addition, early coverage is crucial to reduce the risk of complications, including both additional protein loss and biofilm colonization. With such considerations in mind, we planned skin graft procedures from the beginning, removing unvitalized tissues during the emergency operation. Meanwhile, it is well known that achieving a sufficient range of motion following a skin graft is challenging because of secondary contracture of the grafted skin. Several studies have attempted to use ADM during skin grafts as a viable option for preventing postoperative scar formation and joint movement restriction [10]. Recent studies have reported favorable cosmetic and functional outcomes when ADM (Matriderm) and meshed skin (1.5 to 2:1 ratio) were used for skin grafts [11,12]. In our study, a 3:1 ratio of meshed skin was used, and good outcomes were obtained without complications such as skin loss. Also, the progress of joint movement improved on its own during the rehabilitation program.
When treating a patient with a degloved wound, it is necessary to evaluate the patient's general condition as well as the wound itself, because the wound is inextricably linked to the patient's general condition. For example, the oldest patient, case 2, found it difficult to walk even after achieving full recovery because of her poor general condition. Meanwhile, psychiatric problems should be checked in patients with these injuries. PTSD is a debilitating mental illness that has a negative effect on the health and quality of life of trauma patients. According to Joseph et al. [13], patients who are hit by cars have significantly higher rates of PTSD than those who are not. McCarthy et al. [14] reported that lower extremity injuries have a higher incidence of PTSD due to longer hospitalization. Therefore, patients who have entire lower extremity degloving injuries are more likely to develop PTSD and require mental support during hospitalization and follow-up care after discharge.
Our study has several limitations. First, we could not demonstrate the efficacy of our treatment strategy through comparison because all patients were treated equally. Second, although rehabilitation treatment often takes years to improve disability, we examined only a 4- to 6-month follow-up period.
In conclusion, we established a treatment strategy for patients with entire lower extremity degloving injury using a comprehensive approach and achieved satisfactory results. Therefore, we propose that the strategy described in this study could be useful in patients with entire lower extremity degloving injuries.





