Introduction
High-pressure paint gun injuries to the hand can occur during painting work. As their incidence is low, surgeons who encounter such cases are often unsure of how to proceed in management [1]. In general, the entrance wound observed on the skin is small, but a very large amount of paint inserted by the high pressure of the impact is present underneath the skin [2]. Inappropriate treatment underestimating the wound can result in serious functional deficits of the hand [2,3]. In this case report, we present the appropriate treatment and reconstruction of a high-pressure paint gun injury of the thumb. The patient provided written informed consent for publication of this case report.
Case
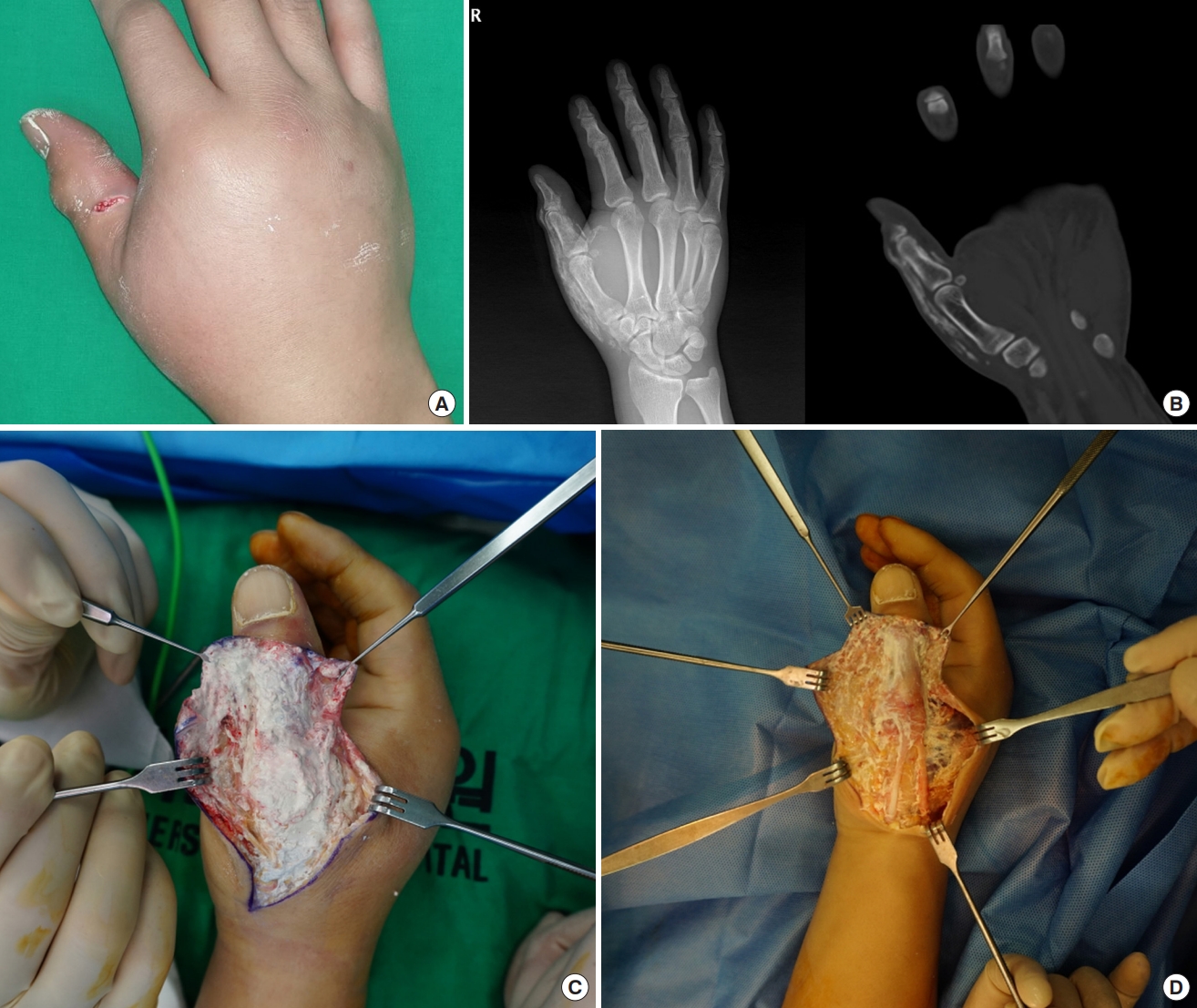
A 39-year-old male patient with a high-pressure paint gun injury on his right thumb visited the emergency room and was referred to the department of plastic and reconstructive surgery. There was a small wound opening on the ulnar side skin of his right thumb, and the interphalangeal and metacarpophalangeal joint of thumb could not be actively flexed. Light touch sensation of the injured thumb was less than half compared to the uninjured thumb. X-ray imaging and computed tomography were performed, showing extensive paint spread along the extensor pollicis longus and brevis tendons without involving the joint spaces (Fig. 1). An emergency operation was planned to remove the paint before it set. Through an additional skin incision along the thumb, as much paint was washed out as possible by irrigation, rubbing with gauze, and minimal debridement. However, complete removal was impossible, as the paint was not fully soluble in water. A large amount of paint was removed, leaving the extensor tendons intact, and the wound was closed after inserting a negative suction drain.
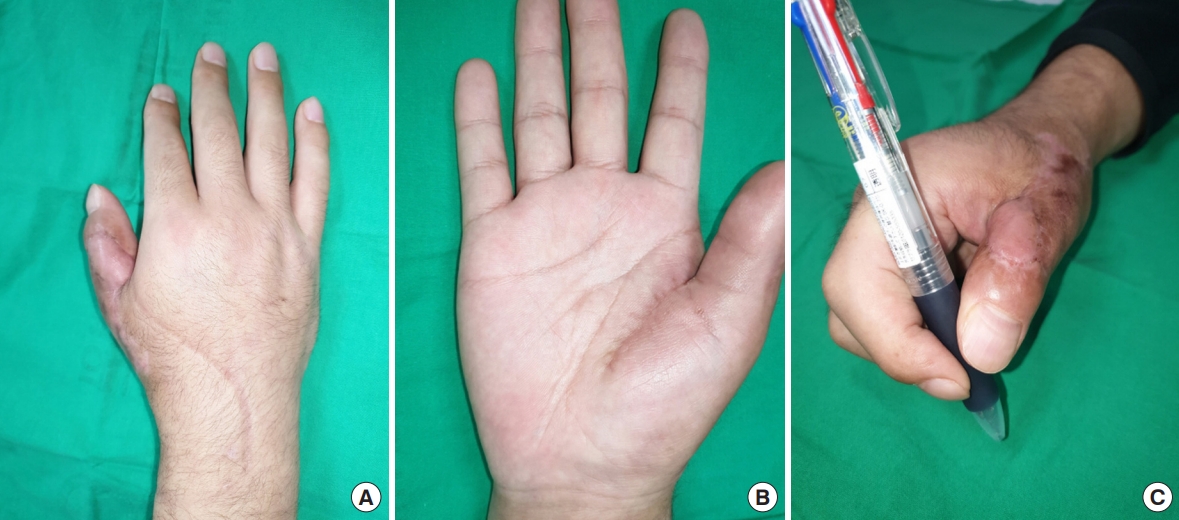
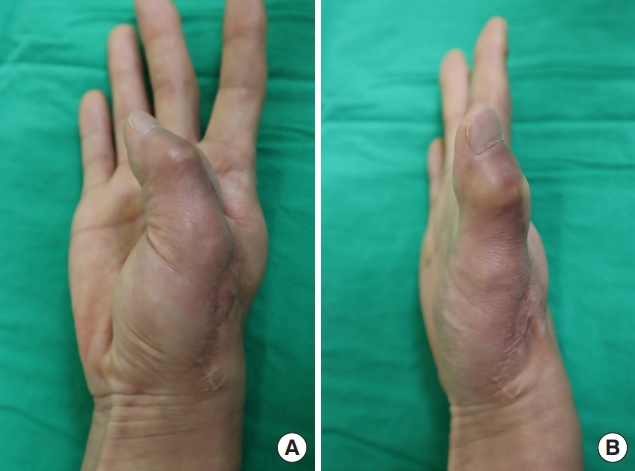
After 6 weeks, the wound was stabilized except for an unhealed defect on the interphalangeal joint (Fig. 2). Active movement of the thumb interphalangeal and metacarpophalangeal joints was still limited. The remaining defect was 2.5×1.5 cm in size with exposure of bone and tendon, and had to be resurfaced with a sufficiently durable tissue flap. For this reason, a reverse thenar perforator-based island flap was planned. An island flap of the same size as the defect was designed on the ipsilateral thenar region. The island flap linked to the princeps pollicis artery through perforators was elevated and moved to cover the defect, and the donor site on the thenar region was primarily closed. The flap had a reverse flow pattern but survived without any complications. At 2 months after flap surgery, the patient recovered pinching and grasping function of his thumb (Fig. 3). Sensory function improved to normal ranges 1 year after the injury. However, in spite of steady exercise, active movement of the two thumb joints remained slightly limited even at 4 years after the injury (Fig. 4).
Discussion
High-pressure paint gun injuries of the hand are often underestimated due to their small external wounds [2,3]. However, large amounts of paint are injected under the skin by the high pressure of the spraying machine. The penetrated paint increases tissue pressure by inflammatory responses. This may lead to compression of neurovascular bundles and can eventually require amputation [4,5]. In spite of surgical removal of the paint, remnant paint can result in tendon injuries and poor wound healing of the skin. Paint gun injuries of the thumb have especially serious outcomes, because the thumb accounts for a large proportion of hand function. The severity of paint gun injuries is related with the type, toxicity, volume, and viscosity of the material injected. The outcome of overall high-pressure injection injuries including paint gun injuries is affected by various other factors including the injection pressure of the injury, involvement of synovial sheaths, functional importance of the involved tissue, presence of secondary infection, and time interval between the injury and medical care.
The most important aspect of treatment for paint gun injuries of the hand is immediate removal of the paint [6,7]. Paint under the skin solidifies over time, which makes it hard to remove from the adjacent structures. Additional skin incisions to expose the paint are needed, and massive irrigation should be performed. If the paint is not water-soluble, it should be removed by thorough rubbing with gauze. A goal of this procedure is to remove as much paint as possible without injuring the tendons.
However, complete removal is often impossible due to the hydrophilic nature of paint which prevents it from completely dissolving in water [8]. The paint in this case was water-soluble but it could not be washed out because it contained various other materials (Table 1). Remnant paint interferes with wound healing of the overlying skin, which often leaves an inevitable defect. When a skin defect occurs with the exposure of structures such as bone or tendon, reconstructing the defect with an appropriate option is essential.
In this case, a reverse thenar perforator-based island flap was used for the reconstruction. Among the many local flaps available in the hand, the reverse thenar perforator-based island flap is well known as an appropriate option for covering thumb defects [9]. An island flap based on a perforator of the princeps pollicis artery can be harvested in the thenar region. One or two cutaneous perforators from the princeps pollicis artery supply the radial aspect of the midpalm with little anatomical variation [10]. Meticulous dissection of the princeps pollicis artery from proximal to distal fashion is necessary. Dissection should be performed until a sufficient length of the pedicle for flap transposition is obtained. With sufficient pedicle length for easy transfer, the flap can cover defects on either the volar or dorsal side of the thumb. As this flap is supplied by retrograde flow of the princeps pollicis artery, it can be considered risky. However, previous studies have shown that the reverse thenar perforator-based island flap is safe enough for use [10,11].
In a high-pressure paint gun injury of the thumb, we conclude that immediate surgical removal of the paint is required and that the reverse thenar perforator-based island flap is a good choice for reconstruction of remnant defects around thumb. The flap is secure with less anatomical variations, provides sufficient pedicle length, and allows primary closure of the donor site.