Introduction
Chronic wounds have a profound effect on both patients and medical systems. In the United States, it is estimated that chronic wounds affect 6.5 million patients and cost the medical system over US $25 billion annually [1]. This expense is rapidly growing due to an aging population and increased incidence of diabetes and obesity. Older patients and shortened hospitalization periods have led to a rise in home care. Currently, various medical devices are used in home settings. These devices are more user-friendly, lighter, and smaller than conventional devices.
Debridement, or removal of non-viable tissue to expose healthy, perfused tissue, is a crucial process in chronic wound care. Necrotic debris acts as a reservoir for infection and impedes wound healing, and thus must be removed in all cases. Debridement can be performed using a variety of techniques, including both autolytic and surgical mechanisms. The optimal timing and frequency of surgical debridement should be tailored to each wound.
Ultrasonic therapy is a relatively painless debridement modality that uses sound waves with a frequency at or above 20 kHz. It preferentially eliminates necrotic tissue, decreases bacterial counts, and minimizes blood loss [2]. In the past few years, use of ultrasound in wound care has increased. Diabetic ulcers, venous ulcers, and other complicated wounds have been treated using ultrasonic therapy [2-4].
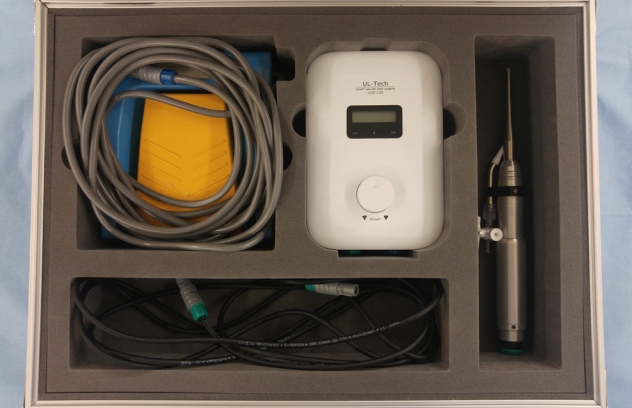
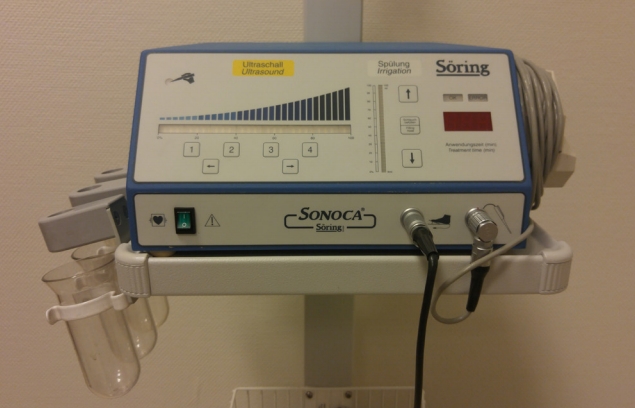
Two current devices for low-frequency ultrasonic therapy are ULSC-12D and SONOCA 180. ULSC-12D is a lightweight and compact ultrasound surgery system lending itself to portable uses (Fig. 1). Its handpiece and main system weigh 196 g and 0.5 kg, respectively. It produces an ultrasound of 25 kHz with a maximum amplitude of 70 μm. SONOCA 180 is an ultrasound surgery system used worldwide (Fig. 2). Its handpiece weighs 147 g, but its main system is a sizable 13.5 kg. It produces an ultrasound of 20 kHz with a maximum amplitude of 140 μm.
We compared the efficacy and safety of ULSC-12D with the conventional SONOCA 180 system in a multicenter randomized controlled clinical trial. We also performed in vitro studies to evaluate the effects of these ultrasound systems on cellular responses relevant to wound healing.
Methods
Clinical trial
A multicenter, randomized, controlled study was carried out with two groups: the study group undergoing debridement using ULSC-12D (Ul-tech, Uiwang, Korea) and the control group undergoing debridement using SONOCA 180 (Söring, Quickborn, Germany). It was conducted at three medical institutes from February to November 2013. A total of 30 patients with pressure ulcers were recruited and enrolled according to the inclusion and exclusion criteria (Table 1). In detail, patients with a stage 2 or greater pressure ulcer sized at least 3 cm² requiring debridement were included, but patients with signs of cellulitis or other comorbidities hindering proper assessment were excluded. Cognitive diseases that induce an inappropriate response and spinal diseases that induce a lack of sensitivity were examples of such comorbidities. Except for simple dressing changes, patients with wounds treated in 2 weeks were also excluded. The patients were randomly allocated to two groups with 15 patients per group.
All the patients were evaluated for intra-procedural pain and post-procedural reduction of bacterial load and necrotic tissue. The procedures were done without anesthesia. Pain was assessed on a visual analog scale. Both bacterial load and the extent of necrotic tissue were measured before and 30 minutes after debridement. Bacterial load was measured using 5×5 cm nitrocellulose membrane filters gently pressed to the center of the wound and immediately inserted into a Columbia Blood Agar plate. Bacterial load was measured by counting the number of individual colonies on the plates after incubating at 37°C for 16 hours. The extent of necrotic tissue was measured using OpSite Flexigrid and Visitrak (Smith and Nephew, London, UK).
The clinical trial was approved by the institutional review board and ethics committee of Seoul National University Bundang Hospital, Samsung Medical Center, and Hanyang University Hospital. It was registered at ClinicalTrials.gov (Identifier: NCT02007824). Informed consent was obtained for all patients.
Primary fibroblast and endothelial cell culture
Human skin fibroblast culture was established using explants from the dermis of adult foreskin. Fibroblasts were cultured in complete Dulbecco’s modified Eagle’s medium supplemented with 10% fetal bovine serum (FBS), 2 mM L-glutamine (Sigma Chemical Company, Saint Louis, MO, USA), and 1X Antibiotic-Antimycotic (Gibco Life Technologies, Grand Island, NY, USA). The cells were subcultured when approximately 90% confluent. Primary endothelial cells were obtained from human umbilical veins, subcultured, and maintained in a 0.2% w/v gelatin-coated 25 cm2 culture flask with complete McCoy’s 5A medium (Flow Laboratories, McLean, VA, USA) supplemented with 20% FBS, 50 mg/mL endothelial cell growth supplement (Collaborative Research, Bedford, MA, USA), and 100 mg/mL heparin (Sigma Chemical Company) until reaching confluence, within 4 to 5 days. Endothelial cells were seeded in a 6-well plate coated with 0.2% w/v gelatin. Cells were cultured in a humidified incubator at 37°C and 5% CO2 and used at passages 3 to 6 for all experiments. For all in vivo assays, there were three experimental groups: treated with ULSC-12D, treated with SONOCA 180, and untreated (control).
Cell proliferation assay
The WST-8 cell proliferation assay was performed on each fibroblast group. When reduced by intracellular dehydrogenase, water-soluble WST-8 [2-(2-methoxy-4-nitrophenyl)-3-(4-nitrophenyl)-5-(2,4-disulfophenyl)-2H-tetrazolium sodium salt] forms a yellowish product (formazan), which is used to measure the number of viable cells.
Collagen synthesis assay
Collagen synthesis was measured by an immunofluorescence technique using a monoclonal anti-collagen antibody. The anti-collagen antibody was obtained by immunizing mouse splenocytes with human collagen. The anti-collagen antibody was labeled with a fluorescent marker and collagen synthesis was measured in each group of human fibroblasts after ultrasound exposure.
Growth factor assay
Growth factor expression was measured by reverse transcription polymerase chain reaction. Expression levels of basic fibroblast growth factor (bFGF), platelet-derived growth factor (PDGF), and granulocyte macrophage colony stimulating factor (GM-CSF) were measured in each group of cultured fibroblasts after exposure to each device.
Nitric oxide assay
Nitric oxide is a highly reactive free radical gas and oxidizer, which remains stored in tissues as nitrate or nitrite. A colorimetric Griess reaction was used to quantify the combined concentration of nitrate and nitrite. Quantitative analysis of nitric oxide production was performed in each endothelial cell group after ultrasound exposure.
Results
Clinical outcomes
The reduction in bacterial counts after debridement was 96.3%±6.7% (mean±SD) in patients treated with ULSC-12D, and 91.6%±16.2% in patients treated with SONOCA 180. The extent of the necrotic tissue was reduced 27.1%±8.1% (mean± SD) post-debridement with ULSC-12D, and 15.1%± 18.2% with SONOCA 180. The differences between groups did not reach statistical significance, however there was a trend toward improved outcomes using ULSC-12D. The average intra-procedural pain assessment score was 5.4 in the ULSC-12D group, and 4.8 in the SONOCA 180 group. This difference was also statistically insignificant, suggesting both devices have comparable efficacy. No significant adverse event was reported in either group during the study (Table 2).
Experimental study
The proliferation rate of fibroblasts was 122.48%±7.11% (mean±SD) in the ULSC-12D group, 110.38%±2.46% in the SONOCA 180 group, and 98.23%±2.47% in the control group. The groups treated with ultrasound were significantly more proliferative than the control group, but the difference between the two ultrasound treatment modality groups was not significant. The collagen synthesis of fibroblasts was 14.53±1.94 μg/mL (mean±SD) in the ULSC-12D group, 6.23±1.48 μg/mL in the SONOCA 180 group, and 1.53±0.22 μg/mL in the control group. The ULSC-12D-treated fibroblasts showed significantly higher collagen production than the other two groups. Expression of bFGF also increased significantly in ULSC-12D group, but there was no significant change in the expression of PDGF or GM-CSF or any growth factors tested in other groups.
Nitric oxide production of endothelial cells was 3.90±0.63 μM (mean±SD) in the ULSC-12D group, 3.32±0.27 μM in the SONOCA 180 group and 2.65±0.25 μM in the control group. Ultrasound treatment significantly enhanced nitric oxide production by epithelial cells compared to the control group, and the effects of ULSC-12D and SONOCA 180 were equivalent (Table 3, Fig. 3).
Discussion
ULSC-12D is as effective and safe as the more conventional SONOCA 180 for wound debridement. Both devices provided acceptable necrotic tissue and bacterial reduction, and no significant adverse events were reported. In in vitro studies, fibroblast proliferation rate and endothelial cell nitric oxide production were significantly higher in ultrasound-treated cells. These laboratory results are consistent with the previous reports.
Ultrasound is a type of sound wave with a frequency greater than 20 kHz, which is out of the range of human hearing. It is widely used not only for diagnostic, but also for therapeutic purposes. Therapeutic ultrasonic devices can be classified by frequency. Low-frequency devices generate ultrasound ranging between 20 and 60 kHz. High-frequency devices mainly function through the thermal and mechanical effects that occur as tissue absorbs ultrasound. Heat promotes wound healing by promoting blood flow to the tissue [5]. Shear forces induced by the rupture of microbubbles stimulated by high-frequency ultrasound also contribute to necrotic tissue destruction [6]. On the other hand, low-frequency ultrasound devices function through biostimulation, which occurs when the mechano-acoustic effects of low-frequency ultrasound are translated to cellular and tissue level biological responses [4]. Both ULSC-12D and SONOCA 180 generate low-frequency ultrasound.
Therapeutic ultrasound at an appropriate dosage has been reported to induce cell proliferation, protein synthesis, and cytokine production by fibroblasts, osteoblasts, and monocytes [4]. Consistent with the previous reports, fibroblast proliferation rate and collagen synthesis were significantly higher when exposed to ultrasound. Particularly, ULSC-12D produced a stronger effect on collagen synthesis than SONOCA 180. Collagen plays a crucial role in wound healing by replacing the initial fibrin-fibronectin clot. It creates an environment appropriate for healing through the regulation of inflammation, angiogenesis, and tissue remodeling [7]. Therefore, it is speculated that ultrasonic surgery systems promote wound recovery by promoting collagen synthesis, and ULSC-12D may be superior to SONOCA 180 in that aspect.
Nitric oxide is a soluble gas continuously synthesized in endothelial cells. It has a wide range of biological properties including modulation of vascular tone [8]. Ultrasound was reported to improve tissue perfusion via a nitric oxide-dependent mechanism, by promoting nitric oxide synthase activity in endothelial cells [9,10]. In our study, nitric oxide production of endothelial cells was significantly higher in cells treated with ultrasound, consistent with the hypothesis that ultrasound increases blood flow through its actions on endothelial cells.
The prevention and treatment of wound infection are important concerns in wound management. There are several reports suggesting that therapeutic ultrasound suppresses wound infection. A reduction in bacterial load of diverse bacteria was demonstrated by in vitro tests, an animal study and a clinical trial [11]. In vivo experiments on simulated implant infections also showed that bacteria were significantly reduced when aminoglycosides were used in combination with ultrasonic therapy [12]. Similar findings of enhanced effectiveness of gentamicin in combination with ultrasound have been reported [13,14]. Both ULSC-12D and SONOCA 180 showed bacterial reduction rates of more than 90% in the clinical trial. The difference between the two devices was not statistically significant, but the standard deviation for ULSC-12D was less than half that of SONOCA 180, suggesting that more consistent results might be achieved using ULSC-12D.
In conclusion, we have conducted a comparative clinical trial between two ultrasonic surgery systems and performed relevant in vitro studies of their cellular-level effects. Taken together, the use of ULSC-12D is as effective and safe as SONOCA 180 for the treatment of chronic wounds. In some respects, ULSC-12D may yield improved results over SONOCA 180. The small size of ULSC-12D is also an advantage and may support an application for its use in the home care of chronic wounds.